Many parents are concerned not only with the psycho-emotional development of the child and issues of general health, but also with such particular issues as, for example, the development of the child’s dental system. In many countries around the world, such attention is a common part of the dental culture, combining prevention, hygienic care and regular follow-up with appropriate specialists. Russia, unfortunately, is not in first place in terms of development of dental culture. In this article we will tell you more about the growth of a child’s jaws, possible developmental anomalies, what and at what age you need to pay attention, and which specialists you should contact if you notice any abnormalities.
The human maxillofacial apparatus develops along with the growth of the child and goes through various stages of development. Thus, the growth of the alveolar processes in width ends around 3 years of age. At this time, you can show the child to an orthodontist so that he can determine the presence or absence of any dental anomalies. By the age of 3, children usually finish erupting their baby teeth. From this moment on, the width of the alveolar processes no longer changes. Further, the alveolar processes will only lengthen. This process usually occurs between the ages of 6 and 12 years, when children's molars erupt.
The bite is formed in stages: temporary – replaceable – permanent.
Temporary milk bite
A primary dentition is a dentition made up of baby teeth. These teeth received this name because of their milky white color. The eruption of baby teeth begins around 6-8 months (earlier and later eruption is possible).
The appearance of the last baby tooth occurs at about 2 and a half years of age. There are a total of 20 teeth in the primary occlusion - 10 each on the upper and lower jaws. In the primary dentition, space is prepared for future permanent teeth: thus, at the age of about 5 years, the spaces between the incisors widen.
A panoramic image (orthopantomogram) shows not only grown teeth, but also the presence of the rudiments of permanent teeth.
Upper jaw
The upper jaw (in Latin - maxilla) occupies a central place among the bones of the facial part of the human skull. This bone structure has a complex structure and performs a number of vital functions.
INTERESTING : As their work activity developed, ancient people transferred some of the grasping functions from the jaw to their hands. As a result, the size of this bone structure has decreased significantly
Functions and purpose
The upper jaw bone performs a number of important functions. Below is a description of some of them:
- Shape-forming. Forms the nasal and eye cavities, the partition between the mouth and nose.
- Aesthetic. The size and shape of this bone will determine the oval of the face, the setting of the cheekbones, and the external attractiveness of a person.
- Respiratory. Forms an extensive maxillary sinus, in which the inhaled air is moistened and heated.
- Chewable . The teeth located on the jaw ensure chewing of the food consumed.
- Swallowing . The muscles and ligaments involved in the process of swallowing food (including the tongue) are attached here.
- Sound-forming. Together with the lower jaw and air sinuses, it takes part in the formation of various sounds. When this bone structure is damaged, a person’s diction is impaired.
IMPORTANT ! During the day, a person makes about 1.4 thousand chewing movements. When chewing bread, the jaw experiences a pressure of 15 kg, fried meat - 25 kg, maximum pressure - 72 kg
Structural features
The upper jaw bone has a complex structure. It consists of several segments and processes, shown in the following picture.
Below we will consider how the body of the jaw bone is structured and how many interconnected surfaces it consists of.
Jaw body
The anterior surface , located under the infraorbital margin, has a slightly curved shape. On it you can see the infraorbital foramen and the canine fossa.
The posterior surface consists of a tubercle and several alveolar openings for nerves and vessels. Next to the tubercle is the palatine groove.
The orbital surface consists of the lacrimal notch and the infraorbital groove, which passes into the infraorbital canal.
The nasal surface and the anterior surface are isolated from each other by the nasal notch. The main part of the nasal surface consists of the maxillary cleft.
REFERENCE : The fixed upper jaw bone is stronger than the movable lower one. Together with other bone structures of the skull, it protects the brain from injury and bruises.
Processes
The palatine process occupies a significant area of the hard tissues of the palate. It is connected to the second process, located on the opposite side, using a median suture.
The frontal process with its upper side is attached to the nasal region of the frontal bone, its anterior side to the new bone, and its posterior side to the lacrimal bone. The lower edge of the process connects to the body of the jaw. The process has a lacrimal groove and a ethmoidal ridge.
The zygomatic process begins at the outer upper corner of the body and has a lateral location. The upper part of the zygomatic process is adjacent to the frontal bone.
The alveolar process is a bone formation with a complex structure. It includes walls, dental alveoli, interdental and interradicular bone septa.
Mounds
The infratemporal part of the jaw has a convex shape. Its most prominent area is called the “maxillary tubercle” (in Latin - tuber maxillae). At the base of the tubercle there are alveolar openings for blood vessels and nerves. The oblique head of the pterygoid lateralis muscle is attached to the maxillary tubercle.
In international practice, the following abbreviations are used to designate tubercles: PNA (according to French nomenclature), BNA (according to Basel nomenclature) and JNA (according to Jena nomenclature).
Features of blood supply
The maxillary internal artery, or rather its four branches, is responsible for the blood supply:
- posterior superior alveolar;
- infraorbital;
- descending palatine;
- nasopalatine (see the following diagram).
The following table shows which areas the listed vessels supply blood to.
Blood supply to the maxillary bone
| Arteries | Areas to which blood is supplied |
| Posterior superior alveolar | Gums, teeth, alveolar process, mucous membrane of the maxillary cavity, bone walls (posterior, lateral) |
| Infraorbital | Inferior orbital canal, orbit, anterior gums, teeth |
| Descending palatine | Hard palate, pterygopalatine canal, soft palate and surrounding tissues |
| Nasopalatine | Nasal cavity, incisive canal, posterior parts of the nasal septum |
The venous network, which is responsible for the outflow of blood, does not always follow the pattern of the supply vessels. It is represented by parallel veins and venous plexuses. From the pterygopalatine ganglion, blood flows into the maxillary vein, and from there into the external jugular vein. From the plexus of the alveolar process it enters the facial vein, and then into the internal jugular vein.
Teeth
When studying the anatomy of the human upper jaw, one should dwell in more detail on the structure of the teeth. This bone structure contains incisors, canines, premolars and molars.
Below is a brief description of the structure of the teeth of a normal, healthy human upper jaw.
Teeth located on the human upper jaw
| Tooth name | Tooth shape | Number of tubercles | Root structure |
| Central incisor | Chisel-shaped | 3 | Single, cone-shaped |
| Lateral incisor | Chisel-shaped | 3 | Flattened from center to edge |
| Fang | Pointed | 1 | Single, powerful |
| First premolar | Prismatic | 2 | How many tubercles, so many roots |
| Second premolar | Prismatic | 2 | Cone-shaped, compressed front and back |
| First molar | Rectangular | 4 | With three branches |
| Second molar | Cubic | 4 | With three branches |
| Third molar | Cubic | 4 | Short, powerful |
Despite the fact that teeth differ in types (types) and shapes of crowns and roots, their internal structure is the same.
Diseases and pathologies of the upper jaw
Inflammatory processes in the oral cavity can provoke the appearance of cysts on the human jaw - hollow tumors filled with fluid. Cysts are treated in several ways, but surgery is considered the most successful. More information about the treatment of cysts can be found in the article “Treatment of jaw cysts: radicular, follicular, odontogenic and others.” Bone inflammation can lead to osteitis, periostitis or osteomyelitis, the characteristics of which are presented in the following table.
Inflammatory diseases of the human maxillary bone
| Name | a brief description of |
| Osteitis | Bone damage |
| Periostitis | Inflammation of the periosteum |
| Osteomylitis | Bone marrow inflammation |
Periostitis can occur in fibrous, purulent or serous forms, and osteomyelitis - in acute or chronic forms. The listed diseases can cause odontogenic sinusitis - a disease associated with the penetration of infection into the maxillary sinuses.
Among malignant formations of this bone structure, tumors of epithelial origin predominate.
Changeable bite
Between the ages of 6 and 12 years, a gradual change of teeth occurs when baby teeth fall out and are replaced by permanent ones. Doctors call this condition a mixed dentition. If your child is already being seen by an orthodontist, then changing the bite is an important stage, which should also take place under the supervision of a specialist. The process of changing the bite looks like this: the first molar erupts behind the last milk tooth. It is important that baby teeth are healthy - only in this case the change in bite occurs normally.
It is not recommended to remove baby teeth prematurely without special medical indications. It is also not recommended to ignore the treatment of baby teeth, believing that “they will fall out anyway.” The first large permanent molar—the “six”—erupts behind the baby teeth when baby teeth have not yet begun to fall out.
Using a panoramic photograph of the jaws, the doctor monitors the change of teeth, the presence of the rudiments of permanent teeth and the depth of their location.
The Dial-Dent clinic places great importance on dental treatment for young patients. Healthy baby teeth are the key to healthy permanent teeth. In addition, timely and regular observation of the child by a pediatric dentist will allow his dental and orthodontic problems to be resolved in a timely manner. Unfortunately, it is still not uncommon now for a desperate mother to come to the clinic and ask to have her baby’s bad teeth treated under anesthesia. It is difficult for a dentist to understand why the parents did not pay attention to the child’s condition earlier, when the treatment would not have been so difficult and traumatic for the little patient...
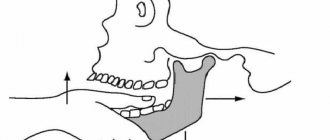
Why does the jaw move forward - how to fix it?
In the structure of dental diseases, anomalies in the development of the dentofacial system today make up a significant proportion. They can affect not only the position of the teeth, but also the structure of the jaws. This causes maximum discomfort to patients, as it deforms the proportions of the oval of the face and seriously affects the appearance. Men and women are equally susceptible to anomalies. Most often, when talking about a protruding jaw, they mean a mesial bite. This anomaly is characterized by the fact that the lower jaw is pushed forward, the lower incisors overlap the upper ones. In some cases, patients are bothered by a protruding upper jaw. In this case we talk about distal occlusion. The lower jaw is inexpressive, the lower lip sinks, and the mouth may look slightly open. The diagnosis is made by the doctor based on the results of an examination of the oral cavity and analysis of x-rays. Sometimes the situation is complicated by crowded teeth. This aggravates the aesthetic problem and can also provoke periodontal disease. The key to proper occlusion is the simultaneous treatment of crowding and distal/mesial occlusion.
Permanent bite
After all primary teeth have been replaced and the second molars (“sevens”) have erupted, the formation of a permanent dentition is considered complete. In an ideal permanent dentition, after changing teeth, the upper incisors should overlap the lower incisors by 2 mm. To assess the correct bite, it is also necessary to pay attention to the relationship and contact of the upper and lower teeth. At this age, your child is most likely already visiting a dentist, who, if necessary, will provide a referral for a consultation with an orthodontist. The last stage of teething will occur at the age of 18-20 years, when wisdom teeth appear. Sometimes there is not enough space for them to grow, or they may be in an incorrect position. In these cases, you may need to consult a dental surgeon.
A person needs a correct bite not only for beauty and beautiful speech, but also for the normal functioning of the maxillofacial apparatus. Poorly chopped food can lead to diseases of the gastrointestinal tract and the entire body as a whole. Over time, malocclusion can cause headaches and poor health. An uncomfortable psychological state also plays an important role for a person with malocclusion. That is why we recommend that you pay attention to the condition of your child’s teeth and promptly listen to the advice of doctors. The sooner you start orthodontic treatment, the better the results will be.
The Dial-Dent clinic has a newly created orthodontic department, headed by orthodontist O.A. Baranova. She specializes in correcting bites in adult patients and solves any, even the most complex cases. If you are concerned about your child’s malocclusion, then it is best to contact pediatric specialist E.V. Rada, the owner of numerous diplomas, certificates and certificates.
Dial-Dent specialists, whom you can contact for advice on the condition of your child’s oral cavity:
- Borisova Yulia Aleksandrovna, pediatric dentist.
- Nazarenko Evgenia Yurievna, pediatric dentist.
- Rada Elizaveta Valerievna, dentist-orthodontist, correction of bite in children.
- Selector Olga Nikolaevna, dentist-orthodontist, bite correction in children.
- Sleptsova Maria Pavlovna, dentist-orthodontist, bite correction in children.
- Tsukor Tatyana Borisovna, speech therapist - child psychologist.
- Smirnova Elena, dental hygienist.
Anatomy of the human jaw
The human maxillofacial region has the following anatomical structure:
- mouth slit,
- vestibule of the oral cavity,
- cheeks,
- lips,
- solid sky,
- soft sky,
- language,
- gums,
- teeth,
- upper and lower jaw.
The oral fissure is limited by the lips, which represent the orbicularis oris muscle and subcutaneous fat.
The cheeks are formed by adipose tissue (Bishat's lump) and bundles of buccal muscle. In the projection of the crown of the upper second molar on the inside of the cheeks there is a papillary elevation of the mucous membrane.
The excretory duct of the parotid salivary gland opens from the papillary eminence.
The oral cavity, cheeks, upper and lower gums and teeth form the vestibule of the oral cavity.
Gums are alveolar processes of the upper and lower jaws, covered with mucous membrane, which cover the teeth in the cervical area.
The mucous membrane of the mouth and the enamel of the teeth are constantly moistened with saliva, which is secreted by paired parotid, sublingual and submandibular glands, as well as many small glands, in a volume of up to 1.5 liters per day. Saliva contains organic and inorganic substances, it contains about 18 amino acids, 50 enzymes, mucin, substances with antibacterial activity (leukins, opsonins, lysozyme).
Saliva promotes the maturation of enamel, remineralization, has a cleansing effect, antibacterial activity and at the same time favors the formation of plaque and tartar.
The hard palate is formed by the palatine processes of the upper jaws and the perpendicular processes of the palatine bones.
The soft palate is formed by muscle fibers covered with a mucous membrane with a large number of mucous glands. On the sides of it there are arches - the palatine lingual and the velopharyngeal, between which there are accumulations of lymphoid tissue, the so-called palatine tonsil.
The tongue is a muscular organ covered with a mucous membrane. Its structure is divided into a wide rear part - root, body, middle part and apex. On the upper mucous membrane of the tongue, there are four types of papillae containing taste buds: filiform, leaf-shaped, mushroom-shaped, and rough.
Upper jaw
The upper jaw is a paired fixed bone. Its structure includes the body, palatine process, frontal process, zygomatic process, and alveolar process.
The palatine process takes part in the formation of the hard palate, the frontal process participates in the formation of the orbit, the alveolar process carries the sockets of the teeth - alveoli, and the zygomatic process attaches the zygomatic bone.
In the body of the upper jaw there is a cavity - the maxillary sinus, containing air and lined from the inside with mucous membrane. In close proximity to it are the apexes of the roots of the large molars (especially the sixth). Therefore, there is a high probability that the inflammatory process that has arisen in the tooth and periodontal tissues can easily spread to the sinus - sinusitis will develop.
Lower jaw
The lower jaw is an unpaired movable bone, shaped like a horseshoe. Its structure includes: a body with dental alveoli; two branches ending in condylar and coronoid processes; the condylar process, which connects with the articular fossa of the temporal bone, participates in the formation of the temporomandibular joint, due to which movement in the lower jaw is carried out.
According to data from dental reference books
A full range of dental services in Istra for adults and children: from consultation to complex operations within one clinic “Doctor Nebolit”
Consultation and appointments daily from 9:00 to 19:00
- +7 (49831) 4-42-12
- Contacts