Due to the thin thickness of tooth enamel, children's teeth are sensitive and at risk of developing caries. In childhood, it is quite difficult to ensure proper oral hygiene. At the same time, the chewing teeth have fissures - natural depressions and grooves in which food particles remain. It is very difficult to remove plaque from fissures, so children who have this feature of tooth enamel are recommended to have the cavities sealed. The specialists of the World of Dentistry clinic perform this procedure with high quality.
Features of the procedure
Fissure sealing is an effective procedure that is performed in the dental office. The main purpose of sealing is to prevent the development of dental caries. During the procedure, the tooth surface is covered with a special sealant, which fills all the cavities and creates a protective barrier for pathogenic bacteria. As a result, caries does not develop on the enamel, and the child’s teeth remain intact. A sealant used as a sealant allows teeth to develop and grow healthy, as well as be fully enriched with essential microelements.
Why is this procedure necessary and is it harmful?
The sealing method involves sealing fissures and other anatomical recesses of healthy teeth with adhesive materials in order to create a barrier to external cariogenic factors. The materials used for these purposes are called dental sealants or sealants. The sealant used in this procedure includes anti-caries substances - fluorine and calcium. These components help nourish teeth, significantly reducing the risk of caries. Therefore, it is necessary to understand that fissure sealing is a very useful and necessary procedure.
Indications for fissure sealing in children
The procedure is carried out in the following cases:
- The presence of depressions and frequently located grooves on the teeth.
- Teeth not affected by caries.
- The child's age is up to 16 years. Before this period, mineralization of tooth enamel still occurs; it contains little calcium and fluoride.
- The enamel is too thin.
- Irregular shape of the natural grooves on the teeth.
- Violations of the arrangement of dental units in a row.
- Insufficient oral hygiene.
Only a specialist can prescribe the procedure after examining the child’s teeth. Fissure sealing is not always possible or appropriate. It is better to carry out the procedure immediately after teething to ensure that there is no risk of developing caries. In this case, sealing is performed in several stages as teeth appear or milk units are replaced with permanent ones.
Preventive actions
To ensure that caries does not bother you for many years, you must take the following preventive actions:
- Buy toothpastes containing calcium and fluoride. Parents can brush their children's teeth with toothpaste from the age of 2, and before that they should simply wipe their teeth with fingertips.
- From the age of 3 you can already use children's electric toothbrushes.
- You need to brush your teeth 2 times a day: in the morning after meals and in the evening before bed.
- When using a manual toothbrush, you need to brush your teeth correctly: the movements should only be “sweeping” - from the gum to the tooth, the toothbrush is positioned at an angle of 45 degrees.
In what cases will fissure sealing be useless?
The specialist will refuse to perform the procedure in the following cases:
- The width of the grooves on the teeth is too wide. In this case, regular hygiene is sufficient.
- The grooves are open and self-cleaning.
- There is lateral caries, which affects a large area of the crown of the tooth and requires treatment.
- A tooth that has not fully erupted.
- Increased salivation, which cannot be eliminated by dental methods.
- Absence of carious lesions on teeth for more than four years. In this case, there is no risk of developing caries.
- Allergic reaction to materials used in the sealing process.
Methods of fissure sealing in children
Your dentist will recommend the best sealing method after examining your mouth. Sealing can be done using one of two methods:
- Non-invasive - no impact on tooth tissue. It is only supposed to cover the tooth with sealant. The non-invasive technique can be used for both permanent and mammary units. The main condition for using this method of sealing fissures is their simple structure and the absence of caries.
- Invasive - before sealing, the specialist expands the fissures, opening them with a drill. This technique is prescribed to those patients whose grooves have a complex shape or are located under the masticatory tubercles. The dentist should also make sure that there are no carious lesions at the bottom of the fissures. A visual inspection may not be sufficient for this purpose. To determine the integrity and depth of the cavities, the presence or absence of caries, additional diagnostic studies may be prescribed:
- Radiography;
- Laser luminescence;
- Photothermal radiometry.
A thorough examination will help the doctor determine the degree of need for the procedure and choose the optimal method of therapy.
Materials used
To close the cavities, 2 types of special dental sealants are used:
- Sealant. The material is a low-viscosity composite resin that is resistant to moisture and enzymes found in saliva. The sealant is a light-curing material and has high fluidity. Thanks to its properties, the composition penetrates deep into the fissures and reliably seals them. The advantage of the material is its ability to strengthen tooth enamel due to its fluoride content.
- Glass ionizer. This is a dental cement that is used for filling teeth and fixing orthopedic products. It is widely used by specialists and is more popular than sealant due to its high adhesive properties, biological compatibility and low elasticity and elasticity. In addition, dental cement saturates tooth enamel with minerals due to the content of fluorine, calcium, aluminum and strontium ions. The disadvantage of this material is its low service life compared to resin.
Sealants may be colored or clear. The latter look more aesthetically pleasing and are used if there is a risk of developing caries after sealing. This is due to the fact that the transparency of the material allows you to notice the onset of pathology development in time and cure it. However, colored sealant is used more often, since it is easier for parents to track its integrity and replace it on time. Also, colored sealing materials are more convenient for dentists, as they simplify the application process and make it more precise.
Also, sealants may differ in consistency. For fissures with great depth, materials with a high degree of fluidity are used. If the recesses are small, then denser sealants are used.
The service life of the sealant is on average 5-7 years. While using the material, you should visit the dentist once every six months for preventive maintenance in order to prevent the development of dental diseases and monitor the integrity of the sealant.
Popular brands of dental sealants include:
- "Fissurite". A light-curing material that comes in regular white, clear and fluoride white. It is characterized by high fluidity, stable structure and high level of adhesion to tooth enamel.
- "Fissulight". It is a light-curing one-component composite that has low viscosity. The advantage of this sealant is resistance to wear and prevention of caries due to its fluoride content. The material is white and transparent. White has 6 shades.
- "UltraSeal XT". A modern version of sealant. It has increased fluidity and contains a component that releases fluorine. It is recommended for patients with reduced resistance of dental tissues to caries, in the presence of a large number of carious lesions, low enamel mineralization, deep fissures and upcoming bite correction.
All sealants are supplied with a compact syringe for easy application of the material.
Non-invasive sealing technique:
A non-invasive technique is used to seal medium or deep open fissures. The open type of fissures means that they are completely accessible for visual inspection (after all, only this guarantees that the doctor will not miss caries in the area of the bottom or walls of the fissure). The non-invasive sealing technique means that we will not use a drill to expand the fissures.
There are 2 options for non-invasive sealing, which we will discuss below. Firstly, this is a mineral fissure sealing technique, and secondly, a non-invasive sealing technique using sealants. Sealants are special sealants (they can belong to three classes of filling materials - glass ionomer cements, composites or compomers).
1) Mineral fissure sealing –
It is carried out using the drug “Enamel-sealing liquid”, which was specially developed for mineral sealing of dental fissures (method of deep fluoridation of teeth). This is a two-component preparation for sequential application to the enamel. The first bottle contains anhydrous magnesium fluoride silicate, anhydrous copper-II fluoride silicate and sodium fluoride, and the second bottle contains highly dispersed calcium hydroxide.
Enamel-sealing liquid:
When applied sequentially, very small particles of calcium fluoride are formed (about 10 nanometers). The resulting crystals are located not only on the surface of the enamel, but also penetrate in large quantities into the smallest defects of the enamel, and even foci of demineralization. In the depths of these lesions, they will be located in a thixotropic silicic acid gel environment, which protects them from being washed out (due to this, they remain inside the enamel from 6 months to 2 years). In this case, the particles will constantly release fluoride ions in a concentration sufficient for remineralization.
The effectiveness of mineral fissure sealing:
- A clinical study (Knappwost et al.) showed the very high effectiveness of this method. It was found that 4-5 years after mineral sealing of fissures in 715 permanent teeth, the fissures remained unaffected by caries in 95.2% of them.
- Scientific work “Comparative effectiveness of deep fluoridation and fissure sealing of the first permanent molars” (authors – Adamchik Yu.A., Varno A.A.).
A clinical study showed that 6 months after mineral sealing of fissures in children aged 6-7 years, fissures remain unaffected by caries in 95.3% of first permanent molars. This study compared mineral sealing with non-invasive sealing using the filling material Fissurit F. So, the preservation of the sealant and its loss (while maintaining healthy intact fissures) was observed only in 29.2% and 25.0% of teeth, respectively, and in other cases fissure caries was observed. Thus, some studies show that mineral fissure sealing may be even more effective than non-invasive sealants in some cases. - Scientific work “Clinical and laboratory justification for the choice of fissure sealing method for permanent and temporary teeth in children” (author – I.V. Kravchuk). The study showed that the use of the deep fluoridation method for the prevention of fissure caries in permanent and temporary teeth in children 6-8 years old allows us to achieve 66.9% and 74.6% reduction in caries growth over 1.5 years.
2) Non-invasive fissure sealing with “sealants” –
Of course, the best materials for non-invasive fissure sealing are composite sealants. One of the most popular representatives of this class of materials is the light-curing sealant “Fissurit F”, which also has the property of releasing fluoride ions into the surrounding tooth tissue. However, composites require preliminary etching of the enamel with orthophosphoric acid, and therefore their use is contraindicated in patients with a low level of fissure mineralization (low AIM).
Non-invasive fissure sealing: Before and After photos
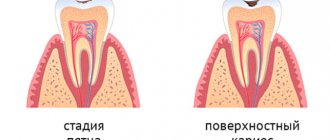
Stages of sealing fissures with composites (Fig. 5-10):
First, the surfaces of the teeth are thoroughly cleaned using a polishing brush and paste (Fig. 5). Next, the tooth is isolated from saliva, after which the surface of the fissures is etched for 15-30 seconds using a gel with 37% phosphoric acid (Fig. 6). After this, the gel is washed off with a stream of water, and the surface of the teeth is dried. Please note that the acid-etched surface of the fissures will have a chalky color (Fig. 7).
Next, a composite sealant is applied (for example, “Fissurit F”) and carefully distributed over all fissures (Fig. 8-9). After applying the sealant, the material must be given 15-20 seconds to flow into the depth of the fissure. Next, the sealant is illuminated for 20 seconds with a polymerization lamp (Fig. 10), after which the chewing surface of the tooth is grinded and polished.
Stages of fissure sealing in the photo:
Indications for non-invasive sealing with composites:
- Erupting and maturing molars with an average level of fissure mineralization (average UIM). Moreover, before sealing the fissures, it would be optimal to carry out a 1-month course of remineralization therapy and/or 3-4 dental fluoridation procedures (at intervals of 5-10 days) to speed up the processes of enamel mineralization.
- Permanent molars and premolars in children and adults – in the presence of a medium or high risk of developing caries.
- Before fixing braces.
Important:
for teeth with a high level of fissure mineralization (high UIM), fissure sealing is usually not recommended (in this case, it is optimal to maintain good hygiene + periodically treat the teeth with fluoride varnish).
Non-invasive sealing of teeth in children (video) –
Non-invasive sealing with glass ionomer cements and compomers –
It must be said that fissure sealing can be carried out not only with composites, but also with glass ionomer cements (GIC) and compomers. GICs have some advantages over composites, for example, they do not require preliminary etching of the enamel, and are also less sensitive to moisture (which is important in young children). However, their disadvantages are insufficient strength, rapid abrasion, insufficiently good marginal fit, and low fluidity.
Most scientific works agree that the use of GIC for fissure sealing may be advisable only in one case - in newly erupted teeth with extremely low fissure mineralization (with low UIM). As for compomer sealants, they are a cross between composites and GIC. The biggest disadvantage of compomers is a very high degree of abrasion; for example, they completely disappear in just 1.5-2 years.
Stages of the procedure
Non-invasive sealing
- Professional oral hygiene using a circulating brush and abrasive paste. Sometimes teeth are cleaned with ultrasound.
- After hygiene, the teeth are treated with an antiseptic solution and thoroughly dried.
- A product containing phosphoric acid is applied to dry teeth. This is necessary for better adhesion of the sealant to the tooth enamel. After a certain time, the product is washed off and the teeth are dried again.
- The sealant is applied and distributed with a special tool along the fissure.
- The sealant is exposed to a light curing lamp.
- After curing, the material is ground and polished.
- At the end of the procedure, the dentist checks the quality of teeth closure with special paper.
It takes approximately 15 minutes to seal one tooth using a non-invasive method.
Invasive sealing
- Professional cleaning.
- If there is caries in the fissures, then local anesthesia is performed.
- The specialist widens the grooves with the help of a bur by preparing them.
- Removal of dental tissues affected by caries and their disinfection.
- Application of light-curing filling material to teeth. Exposure of it to a lamp.
- Grinding and rinsing teeth. Dry them thoroughly.
- Applying sealant. Drying it out.
- Grinding and polishing of teeth, checking the quality of the work performed.
In this case, it takes about 30 minutes to treat one tooth.
Fissure sealing technique
Sealing is carried out according to a certain algorithm:
- first, the doctor thoroughly cleans the tooth surface using fluoride-free paste;
- Next, the fissure is treated with an antiseptic and cotton rolls are installed;
- for better disinfection, the tooth is treated with a special acid, which is subsequently washed off;
- After thoroughly drying the fissure, sealant is applied;
- it is fixed using a lamp;
- the excess is sanded off;
- the surface is coated with a special varnish for greater fixation.
If all steps are carried out correctly, the tooth will remain hermetically sealed for 4-5 years. After this, if necessary, the procedure can be repeated.
Recommendations after the procedure
In order for the sealant to last as long as possible, you should follow the following care recommendations:
- In the first 3-4 hours after applying the sealant, you must refrain from eating so as not to compromise the integrity of the material.
- For the first two days, do not eat solid food, so as not to damage the sealant.
- Carry out hygiene using a soft toothbrush and toothpastes without abrasive particles.
- Do not use an electric toothbrush. This is due to the fact that the high speed of rotation of the bristles negatively affects the structure of the sealant.
- When brushing your teeth, do not press too hard on the chewing surface of your teeth.
Compliance with these recommendations ensures the integrity of the sealant for 5-7 years.
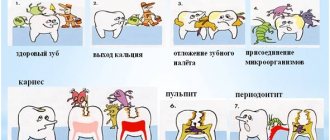
What are dental fissures
There are fissures on both baby teeth and permanent teeth.
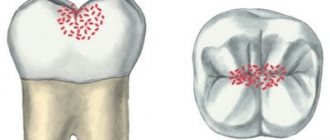
These are physiological folds - grooves, dimples and depressions - on the chewing surface of molars and premolars. The incisors and canines do not have fissures. Such cavities easily and quickly fill with plaque, are poorly cleaned with toothpaste and a brush - they become a common cause of carious lesions. Pediatric dentists often suggest sealing fissures - creating a thin film on the surface of the crown that will protect against pathogenic microflora and mechanical damage.
There are two main reasons for fissure sealing:
- Children's inability to take good care of their teeth. Even the most responsible child is not able to clean all the cavities on the surface of molars and premolars, which leads to the development of caries and the need for treatment. Especially if the grooves differ in depth and tortuosity.
- Thin enamel of teeth - milk and permanent during the period of change of bite. The thickness of the enamel of temporary units is half that of permanent ones, which explains its rapid destruction and susceptibility to caries. During eruption, molars are especially vulnerable - initially the crowns are covered with thin, slightly mineralized enamel, and only after 2-3 years the surface becomes resistant to external damage.
Rodikova Tatyana
Before recommending invasive fissure sealing to a patient, I always look at the initial level of mineralization. With a high mineral content and wide grooves, sealing cavities can be easily done without sealing, but there are cases (low mineralization, prone to caries) when sealing the teeth is the best option!
Advantages and disadvantages of fissure sealing in children
Advantages:
- Effective protection of hard dental tissues from carious lesions
- Saturation of teeth with minerals and essential microelements that promote healthy growth.
- Increasing the strength of tooth enamel.
- Affordable cost of the procedure.
- Safety of the procedure and easy tolerance of sealing materials by children.
- The procedure is painless and there is no need for anesthesia in the case of a non-invasive sealing technique.
Flaws:
- Possibility of malocclusion due to insufficient grinding of the sealant.
- The need to report material after 1.5-2 years.
- Possibility of inhibiting tooth growth.
You can undergo the fissure sealing procedure from experienced specialists at the World of Dentistry clinic. You can make an appointment by calling the phone number listed on the main page of our website.
Invasive sealing technique:
Indications for invasive fissure sealing:
- In the presence of narrow deep fissures in teeth with weak enamel mineralization (if the bottom and walls of the fissures cannot be subjected to visual or instrumental control). In this case, it becomes impossible to guarantee the absence of foci of carious lesions in the area of the bottom and walls of the fissures. In addition, in the presence of deep narrow fissures, it is extremely difficult to achieve good filling of the fissure with filling material.
- Initial fissure caries.
- The presence of pigmented fissures in teeth with weak enamel mineralization (with good enamel mineralization, pigmented fissures do not require mandatory invasive sealing).
Expansion of fissures with a drill during invasive sealing –
Unlike non-invasive techniques, invasive fissure sealing involves expanding the fissures with a drill. In Fig. 11 you can see a section of a tooth, which schematically shows how the fissure is expanded with the help of a bur (within the thickness of the enamel). In Fig. 12 you can see that the deep narrow fissures were expanded using a drill (they are indicated by arrows), after which they were filled with composite material (Fig. 13).
Video of fissure treatment with a drill –