Nimesil and Ketorol are medications that help get rid of inflammatory processes and intense pain. Both medications belong to the group of non-steroidal anti-inflammatory drugs. It is recommended to consult your doctor before choosing the appropriate option.
Nimesil and Ketorol are medications that help get rid of inflammatory processes and intense pain.
Differences
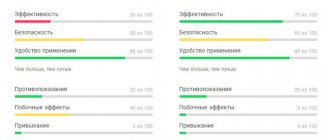
Ketorol is more often used as a pain reliever: its effectiveness against inflammation is lower than that of Nimesil, so doctors prescribe a more effective medicine. Nimesil can be used as a complex remedy; it helps well both with pain and with infectious processes accompanied by hyperthermia.
Various forms of release. Ketorol can be purchased in the form of tablets or solution for intramuscular injection. Nimesil is sold in powder form for the preparation of a solution for oral use.
Nimesil is less likely to cause adverse reactions. This is often taken into account when choosing a pain reliever.
Medicines have different principles of action. Ketorol inhibits the activity of type 1 and type 2 enzymes that synthesize prostaglandins. Such exposure, however, may negatively affect the functioning of the gastrointestinal tract. The second drug affects only the second type of enzymes; the analgesic effect becomes less pronounced.
NSAIDs and triptans for migraine: separately or together?
According to international recommendations, treatment of a migraine attack in most patients should begin with the use of a non-narcotic analgesic or non-steroidal anti-inflammatory drug (NSAID). Placebo-controlled studies in migraine have been conducted for acetylsalicylic acid (ASA) [1–4], ibuprofen [5,6], diclofenac [7–9], metamizole [10], phenazone [11], tolfenamic acid [12], paracetamol [13]. It has been shown that the combination of ASA with paracetamol and caffeine is highly effective for migraine and has advantages over separately used components [14–16]. Intravenously administered ASA relieves migraine attacks better than subcutaneously administered ergotamine [17]. The combination of ASA with metoclopramide was as effective as sumatriptan [18]. Effervescent ASA (1000 mg), ibuprofen (400 mg) and sumatriptan (50 mg) were equally effective for migraine [19,20]. A placebo-controlled study showed that the potassium salt of diclofenac in sachet form (50 and 100 mg) was as effective as sumatriptan (100 mg) in relieving migraine [9]. The selective COX type 2 inhibitor valdecoxib (20–40 mg) also reduced migraine pain [21]. The European Federation of Neurological Societies (EFNS) recommends the use of NSAIDs for the treatment of migraine, the effectiveness of which has been proven in randomized, double-blind, placebo-controlled studies [22] (Table 1). For the relief of migraine, NSAIDs with rapid accumulation in plasma (Tmax) and a short half-life (T1/2) are primarily recommended, which ensures the rapid development of analgesia and the safety of the drug upon repeated use. For this purpose, drugs have been created with modified physicochemical and pharmacokinetic properties, thanks to which rapid analgesia can be achieved (Table 2). Diclofenac, ketoprofen, ketorolac and ibuprofen are most commonly used for the treatment of migraine, since their analgesic activity is higher than that of other NSAIDs [23]. For example, after intramuscular administration of the sodium salt of diclofenac (75 mg) or after ingestion of a sachet of potassium salt of diclofenac (Voltaren-Rapid 50 mg), analgesia occurs on average after 15 minutes. The anise and menthol flavors included in the sachet improve the organoleptic properties of the drug and reduce nausea. A large randomized trial showed that in the treatment of many migraine attacks, the effectiveness of diclofenac potassium salt against headache was comparable to sumatriptan, and associated nausea and vomiting decreased significantly more often than with triptan [9] (Table 3). The clinical effectiveness of triptans for migraine has been demonstrated in large placebo-controlled studies, which are reflected in several published comparative analyses. Triptans are effective during any period of a migraine attack, but their early use increases the effectiveness of treatment [3,15,18]. The use of triptans in the aura phase before the onset of headache is ineffective. The accumulated experience of long-term use of triptans indicates that they should not be used more than 9 days a month, as this significantly increases the risk of transition from episodic migraine to chronic and contributes to the development of abusive headaches. Differences in the clinical effectiveness of triptans are determined not only by the pharmacological parameters of the drugs, but also by the individual sensitivity of the patient. In this regard, if there is no effect from using one triptan, you should not refuse to use another next time. An analysis of 53 studies shows that the effectiveness of triptans taken orally is approximately the same, and only eletriptan at a dose of 80 mg is more effective both overall and in the first 30 minutes. after taking the drug. A comparative analysis of the use of various dosage forms of triptans shows that intranasal and rectal use of these drugs is especially promising for concomitant vomiting. The European Federation of Neurological Societies (EFNS) recommends the use of triptans for the treatment of migraine, the effectiveness of which has been repeatedly proven in randomized, double-blind, placebo-controlled studies [22] (Table 4). Recently, the possibility and feasibility of the combined use of NSAIDs and triptans for the treatment of migraine has been actively discussed and studied. The results of a 2005 study showed that a fixed combination of sumatriptan (50 mg) and naproxen sodium (500 mg) was more effective in relieving migraine attacks than monotherapy with these drugs [24]. Headache relief at 2 hours was significantly greater in patients receiving the fixed combination of sumatriptan and naproxen (65%) than in patients receiving sumatriptan (49%) or naproxen (46%) monotherapy (p<0.01). Complete headache relief in this study was reported in 29% of those taking the fixed combination of sumartriptan and naproxen, 25% of those taking sumatriptan and 17% of those taking naproxen (p<0.001). The comparative effectiveness of rizatriptan (10 mg) and its combination with rofecoxib (25 mg) was studied in 56 patients with migraine. This open-label study showed no statistically significant difference between treatment groups in pain relief and associated symptoms of nausea, vomiting, photophobia, and sound sensitivity. However, the number of patients with headache relapses after its successful relief was significantly (p<0.001) lower in the group of patients taking a combination of rofecoxib and rizatriptan (20%) than in the group taking rizatriptan alone (53%). The authors found no differences between groups in the incidence of side effects [25]. Another study examined the comparative effectiveness of rizatriptan (10 mg) and its combination with rofecoxib (50 mg) and tolfenamic acid (200 mg) in the treatment of six consecutive migraine attacks in 45 patients. Complete pain relief after 2 hours was recorded in 37.9% of patients receiving rizatriptan monotherapy, 40.6% receiving combination treatment with rizatriptan and tolfenamic acid, and 62.9% receiving combination treatment with rizatriptan and rofecoxib. However, 4 hours after the treatment, there were no differences between the groups. The incidence of recurrence of migraine after successful relief was lower with the combined use of a triptan with NSAIDs (15.4% for the combination with rofecoxib and 7.7% for the combination with tolfenamic acid) than with rizatriptan monotherapy (50%) [26]. In 2007, a study was completed that confirmed the high effectiveness of the combination of sumatriptan (85 mg) and naproxen (500 mg) in the treatment of migraine attacks [27]. The authors of these and other studies suggest that the benefit of combining a triptan and an NSAID is due to the complex effects of these drugs on various mechanisms of migraine pathogenesis, as well as differences in the pharmacokinetics of these classes of drugs. The advisability of using NSAIDs during the aura phase, when triptans are not recommended, or early joint use in patients with severe migraine is emphasized. Thanks to the combined use of NSAIDs and triptans, it is possible to speed up the time of onset of analgesia, as well as prevent relapse of migraine (Fig. 1). The accumulated data allows us to formulate a number of provisions that will help increase the effectiveness of treatment of a migraine attack: 1. NSAIDs are effective for migraine and can be recommended for most patients as first-choice drugs. Administration of NSAIDs intramuscularly or in the form of a modified sachet provides a more rapid development of analgesia. If the patient cannot distinguish a migraine attack from a tension headache, then he should take an NSAID. 2. Triptans are highly effective treatments for migraine. They act on the main links in the pathogenesis of migraine and are not analgesics. They should not be taken during a migraine aura. Triptans are the first choice in patients who do not respond to NSAID therapy. There is individual sensitivity of patients to one or another triptan. 3. The combined use of NSAIDs and triptans can more effectively relieve headaches and prevent migraine relapse. 4. If nausea and vomiting are severe, NSAIDs and triptans should be avoided by mouth. Intranasal, rectal or intramuscular routes of administration are preferred.
References 1. Chabriat H, Joire JE, Danchot J, Grippon P, Bousser MG. Combined oral lysine acetylsalicylate and metoclopramide in the acute treatment of migraine: a multicentre double–blind placebo–controlled study. Cephalalgia 1994; 14: 297–300. 2. Nebe J, Heier M, Diener HC. Low-dose ibuprofen in self-medication of mild to moderate headache: a comparison with acetylsalicylic acid and placebo. Cephalalgia 1995; 15:531–535. 3. Tfelt–Hansen P., Henry P., Mulder LJ, Scheldewaert RG, Schoenen J., Chazot G. The effectiveness of combined oral lysine acetilsalicylate and metoclopramide compared with oral sumatriptan for migraine // Lancet. – 1995. – Vol. 346. – P.923–926. 4. Diener HC, Bussone G, de Liano H, et al. Placebo controlled comparison of effervescent acetylsalicylic acid, sumatriptan and ibuprofen in the treatment of migraine attacks. Cephalalgia 2004; 24:947–954. 5. Havanka–Kanniainen H. Treatment of acute migraine attack: ibuprofen and placebo compared. Headache 1989; 29:507–509. 6. Kloster R, Nestvold K, Vilming ST. A double–blind study of ibuprofen versus placebo in the treatment of acute migraine attacks. Cephalalgia 1992; 12: 169–171 7. Karachalios GN, Fotiadou A, Chrisikos N, Karabetsos A, Kehagioglou K. Treatment of acute migraine attack with diclofenac sodium: a double-blind study. Headache 1992; 32:98–100. 8. Dahlof C., Bjorkman R. Diclofenac–K (50 and 100 mg) and placebo in the acute treatment of migraine. Cephalalgia 1993; 13: 117–123. 9. The Diclofenac–K/Sumatriptan Migraine Study Group. Acute treatment of migraine attacks: efficacy and safety of a nonsteroidal antiinflammatory drug, diclofenacpotassium, in comparison to oral sumatriptan and placebo. Cephalalgia 1999; 19: 232– 240 10. Tulunay FC, Ergun H, Gulmez SE, et al. The efficacy and safety of dipyrone (Novalgin) tablets in the treatment of acute migraine attacks: a double–blind, crossover, randomized, placebo–controlled, multi–center study. Function Neurol 2004; 19: 197–202 11. Goebel H, Heinze A, Niederberger U, Witt T, Zumbroich V. Efficacy of phenazone in the treatment of acute migraine attacks: a double-blind, placebo-controlled, randomized study. Cephalalgia 2004; 24: 888–893 12. Myllyla VV, Havanka H, Herrala L, et al. Tolfenamic acid rapid release versus sumatriptan in the acute treatment of migraine: comparable effect in a double–blind, randomized, controlled, parallel–group study. Headache 1998; 38:201–207. 13. Lipton RB, Baggish JS, Stewart WF, Codispoti JR, Fu M. Efficacy and safety of acetaminophen in the treatment of migraine: results of a randomized, double-blind, placebo-controlled, population-based study. Arch Intern Med 2000; 160:3486–3492. 14. Lipton RB, Stewart WF, Ryan RE, Saper J, Silberstein S, Sheftell F. Efficacy and safety of acetaminophen, aspirin, and caffeine in alleviating migraine headache pain—three double-blind, randomized, placebo-controlled trials. Arch Neurol 1998; 55: 210–217 15. Diener HC, Pfaffenrath V, Pageler L. The fixed combination of acetylsalicylic acid, paracetamol and caffeine is more effective than single substances and dual combination for the treatment of headache: a multi–centre, randomized, double– blind, single-dose, placebo-controlled parallel group study. Cephalalgia 2005; 25: 776–787. 16. Goldstein J, Silberstein SD, Saper JR, Ryan RE Jr, Lipton RB. Acetaminophen, aspirin, and caffeine in combination versus ibuprofen for acute migraine: results from a multicenter, double–blind, randomized, parallelgroup, single–dose, placebo–controlled study. Headache 2006; 46: 444–453 17. Limmroth V, May A, Diener HC. Lysine–acetylsalicylic acid in acute migraine attacks. Eur Neurol 1999; 41:88–93. 18. Tfelt–Hansen P., Henry P., Mulder LJ, Scheldewaert RG, Schoenen J., Chazot G. The effectiveness of combined oral lysine acetilsalicylate and metoclopramide compared with oral sumatriptan for migraine // Lancet. – 1995. – Vol. 346. – P.923–926. 19. Diener HC, Eikermann A, Gessner U, et al. Efficacy of 1000 mg effervescent acetylsalicylic acid and sumatriptan in treating associated migraine symptoms. Eur Neurol 2004; 52:50–56 20. Lampl C, Voelker M, Diener HC. Efficacy and safety of 1000 mg effervescent aspirin: individual patient data meta–analysis of three trials in migraine headache and migraine accompanying symptoms. J Neurol 2007; 254:705–712. 21. Kudrow D, Thomas HM, Ruoff G, et al. Valdecoxib for treatment of a single, acute, moderate to severe migraine headache. Headache 2005; 45: 1151–1162 22. Evers, S., Afra, J., Frese, A., Goadsby PJ, Linde M., May A. and Sandor PS EFNS guideline on the drug treatment of migraine – revised report of an EFNS task force. European Journal of Neurology 2009, 16, 968–981 23. Ignatov Yu.D., Kukes V.G., Mazurov V.I. Clinical pharmacology of nonsteroidal anti-inflammatory drugs, M., GEOTAR, 2010,–258 C 24. Smith TR, Sunshine A, Stark SR, et al. Sumatriptan and naproxen sodium for the acute treatment of migraine. Headache 2005; 45:983–991. 25. Krymchantowski AV, Barbosa JS. Rizatriptan combined with rofecoxib vs. rizatriptan for the acute treatment of migraine: an open label pilot study. Cephalalgia 2002;22:309–12. 26. Krymchantowski AV, Bigal ME. Rizatriptan versus rizatriptan plus rofecoxib versus rizatriptan plus tolfenamic acid in the acute treatment of migraine. BMC Neurol 2004;4:10 27. Brandes JL, Kudrow D, Stark SR, et al. Sumatriptan–naproxen for acute treatment of migraine: a randomized trial. JAMA 2007; 297:1443–1454
Contraindications
Nimesil cannot be used for the treatment of intolerance to components, allergic reactions, inflammatory processes in the intestines, fever, viral pathologies, bronchial asthma, recurrent formation of polyps in the nasal cavities, gastric or duodenal ulcers, severe renal, hepatic or heart failure, any pathologies liver. Do not take during pregnancy or lactation. Children under 12 years of age should not be taken. Do not use for alcohol or drug addiction. Do not combine with other NSAIDs.
Ketorol cannot be treated if you have intolerance to the components, allergies, peptic ulcers of the duodenum and stomach, gastric bleeding, inflammatory processes in the intestines, hemophilia, bleeding disorders, cardiac, renal, liver failure, pathologies of the liver and kidneys in the active stage, after coronary artery bypass surgery, before and during surgery, during pregnancy, lactation, and childbirth. Do not use in children under 16 years of age. Do not combine with other NSAIDs containing acetylsalicylic acid.
Recovery immediately after surgery
In the first days after surgery, we recommend that our patients do not travel to another city if possible. Being close to the dentist, you will receive timely medical assistance if necessary.
So, you went home after dental implantation. You may feel slight weakness, numbness from the anesthesia, and minor discomfort in the surgical area. This condition will go away in 3-4 hours, so you do not need to take additional measures.
However, your body will need time to recover for the first 1-2 days. To make this process easy and unnoticeable for your usual lifestyle, we recommend adhering to the following rules:
- For the first day, limit yourself to rinsing your mouth only. The next day, you can brush your teeth with a brush and toothpaste, carefully avoiding the implant installation site so as not to damage the seam.
- Apply a cool compress to the outside of the implanted area. This should be done very carefully to avoid overcooling the nerve near the implant.
- For the first few days, you need to take antibiotics; painkillers are taken according to the condition if there is minor pain. It is also necessary to prevent mechanical impact on the implantation area
- Avoid physical activity after dental implantation, as this may cause adverse effects in the surgical area.
- Take care of your health so as not to get colds. Failure of the immune system and the syndromes that accompany it, such as coughing, sneezing and high fever, can provoke implant rejection.
Side effects of drugs Nimesil and Ketorol
Nimesil can rarely cause anemia, hemorrhage, and pancytopenia. Allergic reactions are possible: itching, skin rashes, redness of the skin, increased secretion of mucus and sweat. Occasionally, dizziness, anxiety, nightmares, headaches, and drowsiness are observed. Possible decrease in visual acuity, increased blood pressure, increased heart rate. Diarrhea, nausea, vomiting may occur, and less commonly, constipation and flatulence. Gastritis and the formation of peptic ulcers are more rare. There may be blood in the urine.
Taking Ketorol can cause stomach pain, diarrhea, gas formation, constipation, vomiting, nausea, cramps, hepatitis, acute renal failure, and frequent urination.
Taking Ketorol can cause stomach pain, diarrhea, gas formation, constipation, vomiting, nausea, cramps, hepatitis, acute renal failure, frequent urination, nephritis, visual and hearing impairment, rhinitis, laryngeal edema, headaches, dizziness, drowsiness, depression, hallucinations, psychosis, fainting, pulmonary edema, hypertension, nosebleeds, anemia, leukopenia, skin rashes, urticaria, pain at the injection site (during injections), swelling, weight gain, increased sweating, swelling of the tongue.
Patient reviews
Oleg, 34 years old, Kharkov: “The doctor prescribed Nimesil for lower back pain. Took it twice a day for 10 days. The condition has improved greatly, the excruciating pain has disappeared. He combined therapy with folk remedies and special massage. The only negative is that the solution has an unpleasant sour taste.”
Elena, 27 years old, Penza: “The doctor prescribed Ketorol tablets because of severe toothache that appeared even at rest. I felt relief after the first use; The low price of the medicine also became an advantage. I took 2 tablets a day for 3 days. Then the diseased tooth was treated, the pain went away completely.”
Medicines in dental practice. Part II
In the last post, we talked about the general principles of prescribing medications in outpatient dentistry. The topic is still relevant, it can be commented on and discussed.
Today I propose to take a more specific look at painkillers and anti-inflammatory drugs in dental practice, and at the end of this post you will find a small gift.
In order not to turn all this into a dull lecture on pharmacology, I will tell you only about those drugs that I use myself and for which I have my own clinical observations.
Attention!
This entry is not a doctor’s prescription, not a recommendation for patients, but a simple information message, a generalization of one’s own experience with medications. Never take medications without a doctor's prescription.
So, let's begin.
General information about pain medications.
All medications that we call “painkillers” (analgesics) can be divided into two large groups.
First group
- narcotic analgesics: morphine, heroin, fentanyl, sodium hydroxybutyrate, etc.
A distinctive feature is the effect, first of all, on the central nervous system (CNS), hence the ability to relieve even very severe pain.
The disadvantages are addiction, sedation, mental or physical dependence, depression of vital CNS centers up to cardiac and respiratory arrest.
In outpatient dentistry, narcotic analgesics are not used. For obvious reasons, drug use should be supervised by a doctor.
Second group
- non-narcotic analgesics: analgin, ibuprofen, butadione, nimesulide, etc.