November 30, 2021
One of the main reasons for the spread of rotaviruses is non-compliance with personal hygiene rules, when transmission of infection occurs through hands, which in turn contaminate dishes, toys, and linen
The pathogen is transmitted through dirty hands, that is, the transmission mechanism is fecal-oral, although airborne droplets are also possible. It can affect people at any age, and the causative agent of rotavirus gastroenteritis is a virus from the order Rotavirus, family Reoviridae. Routes of transmission: contact and household (through dirty hands and household items); aqueous (when drinking water infected with viruses, including bottled water); nutritional (most often when consuming milk and dairy products).
The possibility of airborne transmission of rotavirus infection cannot be ruled out. But one of the main reasons for the spread of rotaviruses is non-compliance with personal hygiene rules, when transmission of the infection occurs through hands, which in turn contaminate dishes, toys, and linen.
The carrier of the infection is a sick person or a healthy virus carrier. The virus multiplies in the cells of the mucous membrane of the gastrointestinal tract and is excreted in the feces for up to 3 weeks (usually 7-8 days from the first symptoms of the disease). Damage to the mucous membrane of the digestive tract disrupts the digestion of food and leads to the development of severe diarrhea and dehydration. The main mechanism of transmission of rotavirus infection is through food. Infection occurs through the fecal-oral route.
Symptoms of rotovirus
Rotavirus or intestinal flu is highly contagious and spreads quickly in confined spaces. If one family member becomes ill, then with a high degree of probability the infection will be transmitted to everyone. Most often, patients complain of dizziness, nausea, weakness, chills, vomiting and diarrhea.
One of the leading symptoms of rotavirus infection is sudden onset of diarrhea.
During the course of the disease, there is an incubation period lasting up to 5 days, an acute period lasting 3–7 days, and a recovery period (4–5 days).
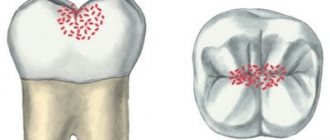
The onset of the disease is always sudden and is characterized by a sharp increase in temperature, as well as repeated increasing vomiting, cramping pain and rumbling in the abdomen, and the development of diarrhea is possible. The nature of the stool helps diagnose rotavirus infection. On the first day of illness, the stool is liquid yellow in color; in subsequent days, the stool becomes gray-yellow with a clay-like consistency. In addition to intestinal manifestations of the disease, patients are bothered by a runny nose, sore and sore throat, and cough.
The frequency of bowel movements often corresponds to the severity of the disease. If you have large, loose stools, dehydration may develop. From the very beginning of the disease, abdominal pain may be observed. More often they are moderate, constant, localized in the upper half of the abdomen; in some cases - cramping, strong. Signs of damage to the digestive organs persist for 3–6 days.
Chronic pain in children: treatment with opioid drugs
Contents "Children's" pain management ladder
Narcotic analgesics – in Russia and in the world
Administration of drugs
A common question parents ask after transferring a child to palliative care is: “How quickly will the pain develop?” This question is difficult to answer, just like the question: “How long does a child have left to live?” We can only predict that more than 90% of children in the terminal period develop chronic pain syndrome. But, for example, in children with brain tumors, especially small ones, it may not be present at all. And the maximum we can use is
is dexamethasone as a drug that reduces intracranial hypertension.
Unfortunately, pain relief for both children and adults is not always adequate for a number of reasons. First, doctors are afraid of the side effects of painkillers. Secondly, some of them are sure that the child will become addicted to opioids. And thirdly, inadequate prescription of painkillers is associated with punitive measures from the administration and inspection bodies.
In 2012, WHO issued recommendations for the treatment of persistent (chronic) pain in children with underlying medical conditions. They begin with the words: “Despite knowledge and tools to relieve pain, in children it is often unrecognized, ignored and even denied.” This is not only a Russian, but also a global problem. According to a survey by the Eastern Cooperative Oncology Group (ECOG), about a third of doctors do not prescribe strong narcotics to a patient if they expect him to live less than six months.
WHO recommendations for drug treatment of persistent pain in children with medical illnesses New two-step approach to drug treatment World Health Organization
Through the efforts of the Children's Palliative and Gift of Life foundations, as well as the Practical Medicine publishing house, WHO recommendations were translated and published in Russia. Previously, doctors used the 1986 WHO recommendations for the treatment of chronic pain. They were common for adults and children and included pain only in cases of cancer. Also, over the years, new drugs have come into use, and some of them have proven to be more effective than previous ones.
Combined synthetic opioid drugs appeared, and unsafe drugs, such as codeine, went out of practice.
"Children's" pain management ladder
According to WHO recommendations, a two-stage “children’s” pain management ladder should be used. The first step works for mild pain: non-narcotic analgesics (paracetamol, ibuprofen) are used. If there is a neuropathic component of pain, then the patient is prescribed an adjuvant.
At the second stage, strong narcotic drugs (in particular, morphine and fentanyl) are used to treat moderate to severe pain, which can also be combined with non-narcotic analgesics. For a neuropathic component, an adjuvant is prescribed. At the second stage of pain relief, short-acting morphine is used. The prerogative is given to drugs used orally. These medications may also be used to treat breakthrough pain.
Codeine is not recommended for children, since up to 47% of patients do not have the enzyme for its transformation in the body - CYP2D6. When prescribing a drug, doctors cannot predict how it will be metabolized. A child with a low metabolic rate may have insufficient pain relief. On the other hand, patients who metabolize codeine at a high rate are at risk for severe opioid toxicity, respiratory complications, and even arrest.
In 2021, the US Food and Drug Administration banned the use of not only codeine, but also tramadol in children under 12 years of age.
This is due to the fact that in the United States there have been deaths of children from respiratory arrest while using tramadol. In addition, there are no randomized studies on the safety and effectiveness of its use. And if for morphine there is an antidote - naloxone, then for tramadol and codeine there are no antidotes. Tramadol is also not licensed for pediatric use in many countries.
Narcotic analgesics – in Russia and in the world
At the end of 2021, the Children's Palliative Foundation prepared a Drug Formulary in Palliative Pediatrics, which lists starting doses of opioids in children aged from a month to a year and from a year to 12 years. This is an adapted edition in Russian, published on the basis of the Association for Pediatric Palliative Medicine formulary. Not all drugs listed in the formularies are approved for use in Russia, but nevertheless, they are important for informing palliative specialists. Recently, a lot has changed, and we now have 2nd line pain relief drugs in our arsenal, which are used in the world when 1st line drugs are ineffective and toxic.
Among the short-acting drugs registered in Russia for the treatment of chronic pain in patients from birth, the following can be used: morphine hydrochloride and fentanyl. If we talk about long-acting drugs, then morphine sulfate (MCT-Continus, Skenan), morphine hydrochloride and fentanyl in patches are prescribed. It is important to note that promedol can only be used to treat acute pain, since the metabolites of this drug are toxic to the body when used for a long time (more than 3 days).
Important
Narcotic analgesics registered in the Russian Federation and used for pain relief in pediatrics:
Morphine sulfate . Capsules, tablets. From 0 years.
Morphine hydrochloride . Injection. From 2 years old.
Tramadol . Tablets, injection solution, suppositories. From 1 year.
Fentanyl . Solution for injection (from 0 years), patch (from 2 years).
For the treatment of chronic pain in children in world practice, according to WHO recommendations, hydromorphone, oxycodone, and methadone can be used in case of ineffectiveness of morphine or complications caused by its use. If we talk about forms, in addition to tablets, in developed countries lozenges, sprays and drops are used for pain relief.
Important
WHO recommends that medicines available for children include:
Solution for injection: 10 mg in 1 ml ampoule (morphine hydrochloride or morphine sulfate).
Granules (extended release): 20 mg, 30 mg, 60 mg, 100 mg, 200 mg (morphine sulfate).
Oral solution: 10 mg/5 ml (morphine hydrochloride or morphine sulfate).
Tablets (immediate release): 10 mg (morphine sulfate).
Tablets (extended release): 10 mg, 30 mg, 60 mg, 100 mg, 200 mg (morphine sulfate).
In 2021, transdermal fentanyl (a patch) appeared on the list of narcotic drugs approved for the treatment of children, which provides pain relief for 72 hours. Fentanyl is prescribed as a second-line therapy for chronic pain when morphine is ineffective or the patient experiences severe intractable complications from its use, such as nausea, vomiting, constipation, itching, and respiratory distress.
Pain relief for a child at the end of life
Pediatrician Natalya Savva on the prescription of analgesics in the last days of life Natalya Savva
Pain relief
The lack of diversity among acceptable drugs and the lack of “children’s” forms of painkillers does not mean that pain in children should be denied or ignored. We have the ability to adequately provide pain relief to children, including children under 2 years of age.
Administration of drugs
The basic principles of pain relief were proclaimed in the 1986 WHO recommendations - “by the hour”, “by mouth”, “individual approach”. This means that the drug must be administered strictly according to the clock, without expecting a decrease in the analgesic effect. The “gold standard” for pain relief is short-acting morphine, which is administered every 4 hours 6 times a day. Administration of the drug every 4 hours is considered the “primary dose”.
Also, pain relief should occur “ascending”: if treatment with first-stage opioid analgesics is ineffective, then move on to strong second-stage opioid analgesics with a gradual increase in dose.
All doses of the drug prescribed to the patient must be recalculated daily, taking into account additional doses taken over the past day. If there were more than 2-3 additional administrations of the drug per day, then when calculating the new daily “main” dose, it is necessary to add the sum of all additional doses taken over the previous day to the “main” dose for the past day.
It is possible to determine which type of anesthesia is suitable for the patient only by examining him. There are patients for whom only the subcutaneous route of administration is possible: the child cannot receive anything by mouth, not even drops.
If the patient is severely malnourished and does not have a developed subcutaneous fat layer, then the drug will not be absorbed when administered subcutaneously - so intravenous administration will have to be prescribed. Intravenous administration is also used if the patient requires high doses of morphine: they cannot be administered subcutaneously due to the high concentration of the drug. When prescribing a drug, it is necessary to examine the patient, talk with him and his relatives, and assess the intensity of pain using scales.
More detailed information on pain management algorithms for persistent pain can be found in the clinical recommendations adopted in 2017 by several professional communities and approved by the Ministry of Health of the Russian Federation.
Recorded by Diana Karliner
Prevention of rotavirus
Nonspecific prevention includes a set of sanitary and hygienic measures (regular hand washing, using only boiled drinking water, room ventilation, wet cleaning). Another important point is the timely isolation of a sick person who exhibits signs of acute respiratory viral infection and intestinal infection.
Gastroenterologists advise taking prebiotics and probiotics as a preventive measure. Probiotics, called “friendly bacteria,” are live microorganisms that aid digestion and improve protection against possible infections. Natural probiotics are found in fermented milk products: organic yogurt and cheeses, miso soup, sourdough bread, and sauerkraut. There are also probiotic supplements that come in capsules or drinks.