All tissues of the oral cavity, both teeth and gums, are interconnected and naturally have a complex structure. Gums, just like teeth, require careful and thorough care. Periodontology is a separate science in dentistry that deals with the study of gum disease. Inflammation from the teeth can spread to periodontal tissue, and vice versa. Therefore, it is so important to maintain careful hygiene of the entire oral cavity and promptly treat any dental diseases.
What it is
Periodontium is periodontal tissue, the main function of which is to hold the tooth in the alveolus. All periodontal tissues are interconnected, so any changes in the functioning of one or another element inevitably affect the functioning of other elements. The periodontal structure includes periodontium, gums, alveolar processes and cementum. Some dental scientists also include tooth enamel, dentin and pulp in its composition.
The term “periodontium” appeared in dentistry a little over a hundred years ago and has since firmly taken its place in modern dentistry, although in Russia the term “took root” a little later, around the mid-30s of the last century. of periodontology deals with a thorough study of the periodontium, its main functions, structure, and possible diseases .
Classification of periodontal diseases Periodontium
Periodontium
(Greek about, tooth) - a complex morphofunctional complex of tissues surrounding and holding the tooth in the alveolus.
The periodontium consists of
:
gums, periodontium, cementum and alveolar processes.
Trophic.
Determined by a well-defined branched circulatory and lymphatic network and the content of various types of nerve receptors
Support-holding function
. It is carried out by the complex structure of the ligamentous apparatus of the periodontium, gums and alveolar process, thanks to which the tooth is fixed in the alveolus. Numerous collagen fibers located between the alveolar wall and the root cementum hold the tooth in a suspended state.
Shock absorbing
. Provides uniform distribution of chewing pressure over the dentition and alveolar process of the upper jaw and the alveolar part of the lower jaw. This is facilitated by the presence of a hydraulic cushion of loose connective tissue, a glomerular network of blood and lymphatic vessels, as well as tissue fluid.
Barrier.
It is determined by the morphological integrity of periodontal tissues, the protective properties of the covering epithelium of the gums, its ability to keratinize, the presence of plasma, lymphoid and mast cells that ensure constant phagocytosis, the content of enzymes and their inhibitors, thiocyanates and other biologically active substances. The protective function of the gums is also manifested in the emigration of leukocytes into the oral fluid, which is carried out mainly by the gingival papillae.
Plastic.
Provides high regenerative ability of periodontal tissues due to the content of fibroblasts, mast cells, cemento- and osteoblasts, adventitial cells, a high level of energy processes and intense transcapillary exchange.
Reflex regulation.
It is carried out by an extensive neuro-receptor apparatus of the periodontal and oral mucosa, which regulates the force of chewing pressure depending on the nature of the food, the usefulness of the dentition, periodontal and mucous membrane.
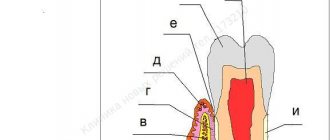
Structure and functions
The periodontal structure includes:
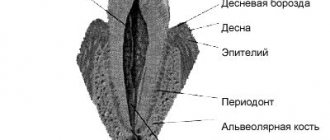
- Desna . Soft tissues that cover part of the tooth root, protecting it from the external environment. The gums are based on collagen fibers, which take an active part in the functionality of the dentofacial apparatus. The soft tissue of the gums is covered on top with epithelium, which has excellent regenerative properties.
- Alveolar process of the jaw . Bone bed of the tooth. It consists of two bone plates, has a spongy structure and is filled with vessels and nerves.
- Periodont . A special connective tissue that fills the space between the alveolar process and the tooth. Consists of special connective fibers, blood and lymphatic vessels, and nerve fibers.
- Cement . Refers to the tissues of the tooth and covers the root of the tooth. Its structure resembles bone tissue.
- Tooth enamel . The hardest part of the tooth, it covers the surface of the crown of the tooth. It is thanks to the hardness of tooth enamel that we can bite and chew food.
- Dentin . Refers to the tissues of the tooth, it is covered with cement and enamel. Dentin is less hard than tooth enamel, it has a huge number of tubules, as well as a cavity filled with pulp.
- Dental pulp . The softest dental tissue, which is responsible for the innervation and nutrition of the tooth. The pulp consists of connective tissue, nerves and blood vessels.
Functions of periodontium:
- Support-retaining . Fixation of the tooth in the alveolus. Thanks to the ligamentous apparatus of the periodontium, alveolar process and gums, the tooth is securely fixed inside the alveolus in a suspended state and does not fall out of its place even under fairly heavy loads.
- Shock-absorbing . Evenly distributes pressure on the teeth and jaw while chewing food. This is facilitated by the presence of connective tissue and tissue fluid, which acts as a natural shock absorber.
- Trophic . It is provided due to the presence of blood and lymphatic vessels, as well as a large number of different nerve receptors.
- Barrier or protective . It is carried out due to the protective properties of the gum epithelium, the presence of lymphoid, plasma and mast cells, the presence of enzymes and other active substances.
- Reflex . It is carried out using the oral mucosa and the presence of nerve receptors in periodontal tissues. Responsible for the force of chewing pressure during eating.
- Plastic . High ability of periodontal tissues to regenerate due to the presence of fibroblasts and osteoblasts.
Blood supply to the periodontium –
The sources of blood supply to the periodontium are the superior and inferior alveolar arteries. In turn, smaller “dental arteries” branch off from them, which already penetrate the apical openings at the apexes of the roots of the teeth. Before penetrating the apical foramen, its alveolar and periodontal branches are separated from the dental artery. The bone wall of the alveoli throughout its entire length is penetrated by a system of perforated canaliculi, through which smaller arterioles penetrate from the alveolar branch of the dental artery to the periodontium.
Periodontal blood supply diagram –
The vascular network of periodontal tissues of adjacent teeth is combined into a single system, which allows for collateral blood flow. An important point is that periodontal vessels can be connected to intrapulpal vessels - through additional openings on the lateral surface of the tooth root. These may be ways for the infection to spread.
The lymphatic system is formed by capillaries that blindly begin in the intercellular substance of periodontal tissue, and is rather poorly developed. From the periodontium of the teeth of the upper jaw, the outflow of lymph occurs into the parotid lymph nodes, and from the teeth of the lower jaw - into the submandibular and sublingual lymph nodes. This is what explains the increase in certain groups of lymph nodes, for example, during exacerbations of chronic periodontitis.
Innervation of the periodontium –
It is carried out from the side of the trigeminal nerve, the afferent and efferent fibers of which form a plexus in the periodontal tissues. The endings of these fibers are pain receptors and mechanoreceptors. In most teeth, the maximum concentration of receptors is concentrated in the area of the root apices, but in the periodontium of the incisors, the receptors are evenly distributed throughout the periodontium. Sympathetic nerve fibers responsible for regulating blood flow are also found in the periodontium.
Etiology and pathogenesis of periodontal diseases
The pathogenesis of periodontal diseases has not been fully established. It is known that at different stages of the development of periodontology, the causes of periodontal diseases such as
- general diseases of the body;
- presence of dental plaque;
- the presence of a large number of aggressive harmful bacteria in the patient’s mouth.
The etiology of periodontal diseases lies in the presence of dental plaque, without which the occurrence of diseases is simply impossible. It is the presence of dental plaque that is the primary factor in the occurrence of periodontal diseases.
Secondary factors include:
- presence of tartar;
- traumatic occlusion;
- the presence of low-quality fillings or dentures in the patient’s mouth;
- anomalies in the position of teeth and bite;
- structural features of soft tissues;
- features of saliva composition;
- genetic predisposition;
- frequent stress;
- hormonal imbalance;
- smoking.
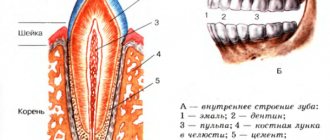
Anatomical and functional structure of the periodontium
The anatomical and functional structure of the periodontium is important for understanding the pathogenesis of the disease and choosing the correct treatment method. But before disassembling the structure of the periodontium, you need to find out what it is. So, periodontium is a collection of periodontal tissues, the main purpose of which is to hold the tooth in the alveolar socket. The periodontium, the structure of the components of which has much in common, can be considered as a single organ.
The structure of the periodontium is as follows:
- ➢ The alveolar process of the jaw is the main component that forms the periodontium. Its structure is the same on both the lower and upper jaws, only on the lower jaw it is called the alveolar part. This is bone tissue that has holes for teeth and acts as a bed for them.
- ➢ Gums are soft tissue that tightly covers the root and neck of the tooth. It consists of connective and epithelial tissue, penetrated by a huge number of vessels and nerves.
- ➢ Periodontium is the tissue located between the compact lamina of the alveoli and the cementum of the tooth. Consists of collagen fibers, blood vessels, nerves.
- ➢ Cement - covers the root and neck, is a type of bone tissue.
- ➢ Dentin is a hard tooth tissue that resembles bone, but unlike the latter, it does not contain blood vessels and is more mineralized.
- ➢ Pulp is a connective tissue containing blood vessels and nerves.
- ➢ Enamel is the strongest tissue covering the crown of the tooth.
This anatomical and functional structure of the periodontium allows us to easily chew the hardest food, but not only - about other functions of the periodontium below.
Differential diagnosis of diseases
The doctor makes a diagnosis based on the results of examining the patient's oral cavity using dental instruments, as well as on the results of an x-ray examination. It is also important to ask the patient in detail about the symptoms, their intensity, and nature. It is very important to conduct a detailed clinical examination of the patient to exclude the presence of other diseases.
Differential diagnosis of periodontal diseases is based on the analysis of radiographic data. With gingivitis, there are no changes in the bone base of the periodontium.
When diagnosing periodontal diseases, so-called indices are often used, which make it possible to determine the degree of the inflammatory process and changes in bone tissue, which allows for the most accurate diagnosis.
Periodontitis
In children, periodontitis is more common, localized in the area of 1–2 or groups of teeth in the frontal area of the jaws with crowded teeth or dental anomalies, with anomalies in the structure and attachment of the frenulum of the tongue, lips, and the small vestibule of the oral cavity. The following signs are characteristic of periodontitis:
- complaints of bleeding gums, sometimes pain in them during exacerbation, bad breath; with initial changes, complaints may be absent;
— symptomatic gingivitis (catarrhal, hypertrophic);
— deposition of supra- and subgingival soft plaque and tartar;
— destruction of the periodontal epithelial attachment;
- formation of periodontal pockets with serous or purulent contents;
— destruction (destruction) of the edge of the alveoli (interalveolar septa), determined on an x-ray;
- exposure of the necks and roots of the teeth;
- tooth mobility and traumatic occlusion.
In the initial form of periodontitis, there may be no complaints; mildly expressed symptoms of catarrhal gingivitis, plaque deposition, false periodontal pockets up to 2–2.5 mm are clinically determined, the teeth are stable, the necks of the teeth are not exposed. X-rays reveal vagueness or destruction of the cortical plate at the apexes of the interalveolar septa and slight osteoporosis of their spongy substance.
In mild forms of periodontitis, patients complain of bleeding gums when brushing their teeth; symptomatic catarrhal gingivitis, small amounts of plaque and tartar deposits, periodontal pockets up to 3.5 mm deep, and slightly or 1st degree tooth mobility are clinically determined. The radiograph reveals the absence of a cortical plate at the apexes and lateral sections of the interalveolar septa, expansion of the periodontal fissure in the cervical region, and subsequently destruction of the interalveolar septa up to 1/3 of the root length; foci of osteoporosis of the interalveolar septa. In the chronic course, osteoporosis is not clearly expressed, and during exacerbation it is diffuse in nature.
In the moderate form of periodontitis, complaints of bleeding gums appear during brushing teeth and eating, symptomatic gingivitis, deposition of tartar and plaque, periodontal pockets up to 5-6 mm with serous or purulent discharge are clinically determined; mobility of teeth of the 1st–2nd degree, exposure of the roots of the teeth occurs. The X-ray shows destruction of the interdental septa from 1/3 to 1/2 of the root length, expansion of the periodontal fissure, osteoporosis is insignificant in the chronic course, and diffuse in case of exacerbation.
Severe periodontitis is characterized by complaints of bleeding and sore gums when brushing teeth and eating. Clinically, symptoms of catarrhal or hypertrophic gingivitis are detected, significant deposits of supra- and subgingival calculus and soft plaque, pockets more than 5-6 mm deep, filled with granulations and purulent contents. The radiograph shows destruction of the interalveolar septa within 2/3 of the root length, diffuse osteoporosis of the remaining bone tissue of the septa, mobility of teeth of the 2nd–3rd degree, exposure of the roots, displacement of teeth and traumatic occlusion.
Diagnosis of periodontitis in children
Examination of a child with periodontitis begins with a study of complaints, medical history and life history. Anamnestic data includes information about the physical and intellectual development of the child, common and infectious diseases suffered and existing at the time of examination. When examining a child, pay attention to his posture, since it is a factor in the full development of the child and a risk factor for anomalies in the development of the dental system.
Examination of the face in front and profile at rest and when closing teeth, during conversation and facial movements allows us to determine functional deviations in accordance with facial characteristics. Thus, the “thimble” symptom in the form of pinpoint retraction of the skin on the chin is a sign of impaired swallowing function. Pay attention to the state of tone of the facial and chewing muscles at rest and during function. The type of breathing (nasal, oral, mixed), the position of the lips (closed, open, tense or atonic), the state of the red border of the lips (color, volume, turgor, architectonics, etc.) are determined, which makes it possible to establish a violation of the basic functions of the dental system and bad habits. The condition of the temporomandibular joint and the lymphoid apparatus of the maxillofacial skeleton is assessed.
A study of the vestibule of the oral cavity allows us to judge its depth, severity and nature of attachment of the labial frenulum to the alveolar process, the state of the mucous membrane covering it, the degree of teething, their position in the dentition and the relationship of the jaws. The depth of the vestibule of the oral cavity is determined by horizontal abduction of the lower lip by the distance from the edge of the marginal gum to the level of the transition of the mucous membrane to the lip. The vestibule is considered shallow if the specified distance does not exceed 5 mm, medium with a depth of 5 to 10 mm, and deep over 10 mm. The area of the attached (alveolar) gum is measured in millimeters, as well as the depth of probing of periodontal pockets using a graduated blunt probe. In addition, the localization of the gingival margin relative to the enamel-cementum boundary (degree of root exposure) and the presence of bleeding upon light probing must be determined.
When examining the oral cavity, the condition of the salivary glands, the position, size of the tongue, the structure and nature of the attachment of the frenulum of the tongue, the shape and relationship of the dental arches, and the presence of crowding of teeth in the frontal area are assessed. The teeth are examined to identify carious lesions, and the quality of the applied fillings is assessed. The mobility of teeth and their occlusal and interdental relationships, the presence of plaque and tartar are determined.
To objectively identify the symptoms of gingivitis and its prevalence, the Schiller-Pisarev test is used, and the degree of gum inflammation is determined using the PMA index. The degree of destructive changes in the periodontium is determined by the periodontal index. Assessment of the hygienic state of the oral cavity is carried out using the Fedorov-Volodkina, Green and Wermillion hygienic indices. It is mandatory to determine the uniformity of the occlusal load using the fingerprint method (occlusiogram), as well as radiographic examination of the periodontium. If X-histiocytosis is suspected, an X-ray examination of the jaws and skull bones is performed.
In addition, a study of the child's developmental history is necessary; conducting clinical blood tests (general, for glucose levels to exclude diabetes), as well as determination of immunoglobulin levels to exclude immunoglobulinemia, a general urine test, and if X-histiocytosis is suspected, for neutral fat. According to indications, cytological and microbiological methods are used to examine periodontal pockets. The child must be examined by a pediatrician, hematologist, endocrinologist, immunologist, pediatric gynecologist, psychoneurologist, etc. in order to identify and treat systemic diseases that may affect the course and outcome of treatment of gingivitis and periodontitis.
Differential diagnosis
Periodontitis must be differentiated from chronic gingivitis and changes in the periodontium with X-histiocytosis, diabetes mellitus, constant and cyclic neutropenia, etc. Some difficulties arise in the differential diagnosis of the initial forms of periodontitis with gingivitis. X-ray data are decisive in this case. With chronic gingivitis, as a rule, there are no changes in the alveolar bone on the radiograph; only in rare cases, with long-term and untreated gingivitis, osteoporosis of the interalveolar septa is observed. When analyzing radiographs, it is necessary to take into account the variability of the shapes of the interalveolar septa in children, as well as the fact that the periodontal gap in the area of the necks of the teeth before the formation of the permanent dentition is wider than in other areas; during the period of teething, the interalveolar septa are not formed, the cortical plate at their apexes is not determined.
When differentially diagnosing periodontitis with changes in the periodontium with X-histiocytosis, one must keep in mind that with X-histiocytosis, along with changes in the alveolar bone, there are foci of bone tissue destruction in the body and branches of the lower jaw. In diabetes mellitus, vertical resorption of the interdental septa with funnel-shaped, crater-shaped pockets predominates, which does not extend to the body of the jaw. With constant and cyclic neutropenia, the process is limited to the interalveolar septa and has clear contours.
With cyclic neutropenia, exacerbation of the process occurs at strictly defined intervals, characteristic of a particular child (usually 21 days) and lasts 4-5 days.
Prepubertal periodontitis
Occurs in children under 11 years of age. The most common form is a generalized one. The disease begins during or shortly after the eruption of baby teeth and is manifested by a violation of the attachment of the gums to the teeth and severe destruction of the alveolar bone, leading to premature tooth loss in children from the age of three. The early and aggressive course is due to the fact that such patients have immune defects - there are few monocytes and polymorphonuclear leukocytes in the blood. All children from birth have decreased resistance to infections, furunculosis, pustular skin diseases, otitis, and pneumonia. The children are pale and have low nutrition. This disease is associated with microorganisms of the bacteroid type: Porphyromonas gingivalis, Actinobacylus actinomycetemcomintans. Infection occurs from parents, the window of infection is from 1 to 3 years. It begins with the primary destruction of the periodontium, while at first there are no symptoms of gum inflammation. Subsequently, the architectonics of the gingival margin changes, the gums seem to recede, the necks of the teeth are exposed, deep periodontal pockets form, and then inflammation develops. X-ray reveals vertical destruction of the alveolar bone. Subsequently, mobility, movement and loss of teeth occur. There are no symptoms of bleeding or pain. There is no tartar, the teeth are covered with a soft plaque. Children first lose their milk teeth, then the process spreads to the rudiments of permanent teeth, they erupt early, similar changes occur with them, and by the age of 14–15 all teeth fall out. However, the pathological process does not extend beyond the alveolar bone. With the loss of permanent teeth, the destructive process in the jaws stops.
The same changes in the periodontium, combined with palmoplantar hyper- or dyskeratosis in the form of cracks on the palms, feet, forearms, and increased sweating, are also observed in Papillon-Lefevre syndrome. There is evidence in the literature that taking tetracycline antibiotics for Papillon-Lefevre syndrome during the primary dentition period prevents the development of generalized periodontitis in the permanent dentition and the loss of permanent teeth.
Pubertal (teenage) periodontitis
There are 2 forms: localized and generalized. Localized pubertal periodontitis is observed in practically healthy children and adolescents without systemic diseases. It is characterized by rapid and severe destruction of the alveolar bone in the area of the first permanent molars, and sometimes the incisors. Clinically, mild inflammation (which may be absent) and a small amount of plaque or tartar are observed. Bone tissue destruction progresses 3–4 times faster than with periodontitis in adults. Currently, this disease is associated with a bacteroid of the Actinobacylus actinomycetemcomintans type. In most cases, it occurs in children whose parents are carriers of this microorganism. It enters the periodontal tissue soon after teeth erupt. The process occurs with minimal inflammatory reaction. The rapid spread of the process is due to the fact that specific microflora not only populates the groove and subsequently the periodontal pocket, but also penetrates deep into the periodontal tissues, including bone tissue, where it is quite persistently preserved. On the other hand, this microorganism has the ability to suppress the chemotaxis of leukocytes, and antibodies in such cases do not have time to form. The periodontium is rarely damaged after the eruption of permanent teeth, since by this time specific antibodies have time to form and exert their protective effect. Previously, this disease was described as local desmodontosis, local monoalveolysis according to Orban.
Generalized pubertal (teenage) periodontitis is rare. In this case, the process often involves the periodontium of both jaws. It is characterized by an aggressive course, rapid and severe destruction of the alveolar bone. It is commonly called aggressive, or rapidly progressive, periodontitis. According to foreign and domestic literature, a large number of facultative anaerobic gram-negative rods, mainly Porphyromonas gingivalis, accumulate in the area of the affected teeth. The most aggressive course is associated with the combination of this microorganism with Actinobacylus actinomycetemcomintans and Prevotella itermedia. It is with this combination that microorganisms exhibit a sharply positive mutual influence.
Vector device in periodontology
The Vector device allows you to quickly and reliably cure patients of many symptoms. It not only helps to get rid of the disease, but also activates the reserve forces of the periodontium, which allows you to avoid many problems in the future. With the invention of the Vector device, periodontics has reached a qualitatively new level of disease treatment. Literally in one visit to the doctor you can get rid of such unpleasant symptoms as bleeding gums, inflammation and soreness of the gums. Moreover, the treatment is almost painless.
The Vector periodontal device was invented in Germany and is most often used to remove dental plaque, which is the main cause of periodontal disease. Using the device, you can also treat the surface of the teeth with ultrasound before fixing the dentures. However, its main purpose is the treatment of periodontal diseases.
If you have suffered greatly from an inflammatory disease, Vector will help replace curettage, which is why the device is often used for osteoplasty and gingivoplasty.
Periodontium, histology
What is periodontium at the microscopic level? Histology is a science that can find out this. Considering the periodontium, histology identifies the following main tissues in its anatomical composition - bone (alveolar process), connective (gingiva, pulp, periodontium), epithelial (covers the gum from above).
Among the cellular elements one can find fibroblasts, osteoblasts, cementoblasts, and epithelial cells. Histology also identifies amino acids, polysaccharides and proteins in the components of periodontal tissue.