The number of allergy sufferers is growing and getting younger around the world.
. One, but very typical example: according to the English publication The Guardian, in the UK alone, the number of cases of hospitalization with anaphylaxis increased by 615% from 1992 to 2012. Moreover, for approximately 27% of hospitalized patients, anaphylactic shock was the first allergic reaction in their lives - before it they believed that they were not sick.
Modern research has revealed a connection between allergies and DNA. A predisposition to an allergic reaction can be inherited from parents, but it can also arise as a consequence of one’s own genetic changes.
Scientists do not yet know why and when hypersensitivity to a certain stimulus “wakes up.” But with the help of allergy tests they can find out to which product (food allergy), chemical substance, plant (hay fever), animal, etc. a violent immune reaction occurs in the body. Such an analysis will help to avoid contact with a potentially dangerous irritant, maintain health and even life.
Allergy tests can also be performed on people who have not had allergic reactions. Tests will help determine what may trigger an unwanted immune response.
Testing is carried out in 2 main ways - using skin allergy tests for a variety of allergens and blood tests. Tests are prescribed by a doctor depending on the purpose of the study, general condition and other factors.
Indications for the study:
- symptoms of food, contact or seasonal allergies are expressed: red spots, itchy rashes, stuffy nose, tears flowing, swelling of the hands, neck, face, oral mucosa, difficulty breathing, etc.;
- hereditary predisposition;
- if treatment of rhinitis, dermatitis, chronic bronchitis, conjunctivitis does not bring results;
- if you cannot tolerate certain foods, medications, or contact with certain animals;
- if you work in hazardous work and cough frequently/constantly, have shortness of breath, rhinitis, or other allergic symptoms;
- if you are undergoing treatment/removal of teeth, surgery with anesthesia.
Go to analyzes
Prescribing allergy tests for children: when and why to do it
Allergen testing is prescribed for children if they have the same symptoms as adults - sneezing, lacrimation, recurrent laryngostenosis, recurring bronchitis, adenoid hypertrophy, etc. If a child gets sick very often, this is also a reason to undergo allergy testing.
But even if an allergy is identified, testing is carried out only when absolutely necessary. If hypersensitivity does not cause any particular concern or complications, the study is carried out no earlier than 5 years of age.
This is explained by the fact that children’s immunity is just developing and there is a high probability that after some time the allergic reaction will change.
But if there is a serious need, skin allergy tests are carried out from 2-3 years of age, when the child can sit quietly for about 15 minutes. There is a special pediatric allergen panel for research:
- epithelium, pet hair;
- milk;
- mites living in house dust;
- egg yolk and white;
- pollen of birch and some herbs;
- other irritants depending on the region, place and lifestyle.
You should be aware that testing often gives false positive results. This is explained by the anatomical features of the child’s skin. The older the person, the more accurate skin tests are.
If the baby requires research (for example, when the parents are allergic), then from 4-6 months a blood test is prescribed, primarily for the level of immunoglobulin E (IgE total). Its increased concentration indicates that the child is prone to allergies. The norm of immunoglobulin E for children and adolescents:
- in children under 2 years of age - 0–64 mIU/ml;
- in children from 2 to 14 years old - 0–150 mIU/ml;
- in adolescents over 14 years of age - 0–123 mIU/ml.
To more accurately determine what the baby is hypersensitive to, a test is performed to determine specific IgE. Blood serum is brought into contact with different types of allergens:
- food;
- household;
- related to rodents, mold, fungi;
- plant pollen;
- others from the pediatric and general panels.
Unlike skin tests, blood tests are less sensitive to non-protein allergens, so sometimes a battery of tests is required.
Basophil Activation Test (BAT)
In recent decades, BAT has been the classic method for diagnosing allergies. Basophils and mast cells play a central role in immediate allergic reactions. DG Ebo [18] points to the increasing interest of researchers in BAT, in which the activation of these cells is measured by flow cytometry. Currently, the most commonly used basophil activation markers are CD63 and CD203c. Flow-CAST and CAST-ELISA are commercial assays based on basophil activation. CAST-ELISA determines the release of sulfodyleukotrienes activated by basophils by ELISA. The analysis is extremely slow and takes a lot of working time; its use is impractical in busy laboratory conditions.
Flow-CAST uses flow cytometry to identify basophils labeled with anti-IgE-fluorescein isothiocyanate and anti-CD63-PE, markers of activation and degranulation. Modification of Flow-CAST using anti-CD203c instead of anti-CD63 improves the performance of the study [25].
The sensitivity and specificity of BAT in allergy to muscle relaxants are reported to range from 36% to 92% and from 93% to 100%, respectively [26], and for allergy to beta-lactam antibiotics, the sensitivity ranges from 33% to 67% and the specificity from 79% to 100% [27]. The BAT method can be considered very promising for the assessment of both immediate allergic reactions and non-allergic hypersensitivity [28]. There is limited experience with the use of the BAT method for drug allergies to LA. So, N.V. Bychkova studied the reactions of 189 people (average age 37 years) to MA groups of articaine, lidocaine, mepivacaine (1:30 dilution). The least sensitization was detected in patients to drugs of the lidocaine (8%) and mepivacaine (3%) group. Among drugs in the articaine group, the frequency of positive reactions in patients varied from 41% to 18%, depending on the composition of the drug. The author concludes that the use of lidocaine, mepivacaine and articaine, which do not contain preservatives, is preferable for patients [29].
Tests for food allergies
A food or nutritional allergy is a disproportionate and unwanted immune response to substances in vegetables, fruits, fish, etc. An allergy to food (as well as to other irritants) does not depend on the amount of food eaten - sometimes a few grams are enough for anaphylactic reactions to develop shock.
About 3% of adults suffer from the disease in an obvious form, in an erased form (they do not associate food and the symptoms after it with allergies, because the symptoms are minor and pass quickly) - about 6% of adults, children under 6 years old - about 8%. It is not yet possible to cure food allergies, but children “outgrow” it, and in adulthood, for many, the disease either becomes erased or does not manifest itself at all.
An allergic reaction to food occurs within 2 hours after ingestion of the irritant food, most often immediately after ingestion. The reaction manifests itself in:
- rash and itching;
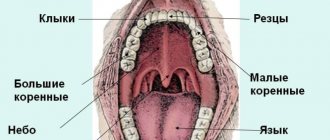
- swelling of the tongue, lips, neck, face;
- difficulty breathing;
- cough;
- runny nose and lacrimation;
- abdominal pain;
- diarrhea of varying intensity;
- vomiting, nausea;
- general weakness, malaise;
- in children, additionally - flatulence, colic, constipation, which are usually combined with an immediate response to the allergen.
The reaction occurs due to an excessive response of the immune system to an irritant in the product. Specific immunoglobulins E are produced. When they interact with proteins, substances are released that can cause negative processes in the gastrointestinal tract, respiratory tract, dermis, etc.
If the allergen enters the body for a long time, immunoglobulins G begin to react and form a delayed, slow reaction. It develops over several hours or even days and usually manifests itself as a rash and itching. The delay makes it difficult to identify the allergen product, and then only tests help make a diagnosis.
Most often, allergies occur to eggs, peanuts, rice, fish, tree nuts, soy products, wheat, and milk protein. In diagnosing an allergen, 2 main methods are used - questioning and laboratory tests:
- general blood test: a reaction to food is often accompanied by an increase in the level of eosinophils—leukocytes;
- determination of the total level of IgE in the blood - in case of allergies it is increased;
- determination of specific immunoglobulins - to determine the specific food component that causes the allergy.
Since a blood test does not allow identifying all allergens, other methods are used:
- keeping a food diary: the patient writes down all meals, scrupulously recording the time, composition, symptoms after consumption (presence, absence, severity, etc.);
- elimination tests (brute force method): a product - a suspected allergen - is removed from the patient’s food and the result is observed;
- provocative tests: when the suspected allergen is removed from the diet, the allergy symptoms have disappeared, the allergen is specially administered to the person, under the supervision of a doctor, and the reaction is observed;
- skin allergy tests: a solution with an allergen is applied to the skin of the forearm, then the skin is lightly scratched (scarification test) or pierced to a depth of 1 mm (prick test), and the reaction is observed.
All these tests are necessary to accurately identify the allergen and eliminate it from food.
Preparation for the procedure
• Tests to determine the reaction are carried out while the allergy subsides. • During the week before the test, if possible, eliminate sources that can cause allergies. • Cancel hormonal and antihistamines two weeks before the test. • Following a hypoallergenic diet, if it was prescribed earlier. Testing performed on an empty stomach may be inaccurate. • To take the test, it is important to refrain from eating 8 hours before the test. • If on the eve of the test you become ill with a viral or infectious disease, the test will have to be postponed.
The patient must strictly follow the doctor's recommendations. Violation of the rules entails false negative or positive results of skin tests. If the result is indeterminate, a repeat study will be required; allergens must be reintroduced, which entails discomfort for the patient.
Allergy tests for anesthetics, antibiotics
Testing for anesthetics and antibiotics has become very relevant. It is carried out before dental treatment, surgical interventions, and special treatment. The importance of such allergy tests is extreme: more and more people react acutely to medications - lidocaine, ultracaine, benzocaine, mepivacaine, diclofenac and others.
A test for anesthetics and antibiotics must be done for those who have:
- an acute reaction to local anesthetics has occurred before;
- any allergy diagnosed;
- there are symptoms of urticaria, itching, cough, lacrimation without an established cause.
To carry out the test, you need to donate blood from a vein. There is no special preparation for testing: 2 weeks before donating blood you need to stop taking antihistamines.
You cannot donate blood for a test if you have a fever, a chronic disease has worsened or an infection has been detected, during pregnancy and after childbirth, or if you have recently had an abortion.
Important!
Testing with a negative result does not provide a 100% guarantee that an allergy to the medication will not occur during treatment. The mechanism of the occurrence of an acute immune response is still unknown to scientists. But the test reduces your risk to an absolute minimum!
Tests for diagnosing delayed allergic reactions to local anesthetics
To diagnose delayed allergic reactions to MA, the following tests are recommended: lymphocyte transformation (TLT); inhibition of macrophage migration; identification of cell membranes; cytotoxicity of lymphocytes; microsomal antibody production [15].
TTL is based on the analysis of T-lymphocyte proliferation in the presence of a causally significant drug allergen. Depending on the drug, the sensitivity of this test is 60–70%, specificity is 85–93% [30].
The clinical picture also determines the sensitivity of the test: for mild and moderate forms of allergic manifestations, sensitivity is higher (58–89%) [31] than for severe bullous dermatitis (25–75%) [32]. Disadvantages include the duration of the test (5–7 days), the need for expensive equipment and well-trained personnel, and the danger of radioactive contamination. Currently, radioactive labels are more often replaced by fluorochromes. However, there are only isolated indications of the use of the TTL method for diagnosing allergy to MA [33]. Increasingly, other, less labor-intensive and less dangerous methods for determining markers of T-cell activation are being used as an alternative to TTL, although TTL is still the “gold standard”.
Immunoglobulin E (IgE) test
IgE are immunoglobulins that are normally found in the blood serum of every person. In adults, the norm is up to 113 mIU/ml. IgE can increase not only with allergies, but also with other diseases, therefore, if the diagnosis is difficult, the doctor may prescribe a comprehensive diagnosis according to indications.
However, even in cases of allergies, the IgE level is not always elevated - in 30% of people with atopic diseases it is within normal limits. In bronchial asthma with an acute reaction to 1 allergen, IgE is normal; only a test for specific IgE and a skin test help diagnose the disease. Angioedema and chronic urticaria do not increase the level of IgE, because in most cases they are of a non-immune nature.
A false negative test result occurs in the presence of antibodies of other classes that are specific to the allergen being tested.
We have given only a few cases where the result of one test may be inaccurate. In reality there are many more. Does this mean that allergy tests are of little effectiveness? No. An experienced allergist will always select a set of tests that will allow you to accurately identify the allergen, and your life will become much safer and more comfortable, because you will know what to avoid.
Laboratory diagnosis of IgE-dependent conditions
Determination of specific IgE
in vitro
is one of the most common methods for diagnosing immediate allergic reactions [19]. For the quantitative determination of allergen-specific antibodies, various methods are used, which are based on the following condition: the allergen, covalently bound to solid particles, is incubated with the patient's serum, presumably containing specific IgE against the allergen under study. Antibodies in the serum bind to the allergen, fixing on particles of the solid phase. The addition of second anti-IgE labeled with various labels (radioimmune, enzyme, fluorescent) makes it possible to quantify the content of allergen-specific antibodies. The advantages of the method include the use of serum, which can be frozen and easily transported. The limitation is the time interval. This method can be used 4–8 weeks after the reaction in patients at high risk of anaphylaxis [20], the intensity of reactions decreases over a year. The method can give false-positive results with high levels of total IgE, but the advantage is the fact of identifying sensitization with a positive history and negative skin tests. The high sensitivity of this method has been proven for beta-lactam antibiotics (38–80%) and neuromuscular relaxants (61–92%) [15].
The authors conducted a study of specific IgE to MA by ELISA using Doctor FOOKE test systems. We examined 280 patients with suspected allergy to LA (questionable medical history and skin test results). Positive tests were detected for: ultracaine - 4.2%, benzocaine - 3.8%, tetracaine - 2.9%, articaine - 2.4%, mepivacaine - 1.9%, bupivacaine - 1.7%, prilocaine - 1 .3%, lidocaine - 4.2% of cases [21, 22].
The authors used the Capture-ELISA option in 147 patients using reagents. As a result, positive tests were revealed for: ultracaine - 3.9%, mepivacaine - 2.1%, lidocaine - 3.8% of cases. The tests revealed a significant correlation with the clinical picture (r>0.5). Considering the possibility of developing allergic reactions to epinephrine, a study of specific IgE for lidocaine, mepivacaine, ultracaine was carried out with the simultaneous determination of antibodies to epinephrine using reagents. Positive tests for epinephrine were detected in 11.8% of cases. Among those examined, 17 people (11.6%) had negative antibodies to MA, and 2 had a positive test for epinephrine. Moreover, these two patients had a history of the development of angioedema and respiratory symptoms (including suffocation) when using the combined drug articaine + epinephrine. Thus, it was concluded that true IgE reactions to MA develop quite rarely, but since these reactions can be life-threatening, studies, including in vitro
, to establish the causative etiofactor, it is advisable to carry out.
It is worth noting the ongoing work towards the development of AllergoFlow, the first domestic test for determining the level of basophil activation using flow cytometry. Since this method can be extremely useful in diagnosing immediate-type hypersensitivity, complex cases of IgE-dependent drug allergies and determining latent sensitization, the company is actively working to expand the range of allergens, including allergens to various MAs, for joint use with test- AllergoFlow system.
IgG study
does not relate to the diagnostic tests themselves and is carried out, as a rule, in combination with the determination of IgE. According to the literature, the role of IgG to allergens is not completely clear. It is believed that there are at least two functionally distinct types of IgG4 antibodies, one of which is blocking antibodies, and the other is anaphylactic. There are studies that have not proven the connection between the presence of specific IgG and IgG4 to the allergen in the blood serum and the clinical manifestations of atopy. However, it is known that IgG characterizes the frequency of contact with an allergen.
The authors studied IgG to MA. As a result, in patients with LA intolerance, IgG was detected for: articaine - 2.4%, mepivacaine - 1.84%, prilocaine - 1%, lidocaine - 4% of cases. The experience gained [23, 24] allows the authors to conclude that the determination of IgG for allergy to LA is an auxiliary diagnostic tool and should be interpreted together with the determination of IgE. When the results of the IgG determination coincide with the results of the IgE determination, then with a high degree of probability we believe that this is an allergic reaction. For the most part, positive results correlate with previous exposure to the drug allergen [25].
Prevention and recommendations
At the beginning of the twentieth century, allergies were a rare disease. And today, the European Academy of Allergy and Clinical Immunology (EAACI) predicts that by 2025, 50% of Europeans will suffer from at least 1 type of allergy.
Scientists associate this incredible leap with the sterility of life of modern man and the poor environmental situation in all its manifestations: the state of air, water, food, excessive enthusiasm for household chemicals, medicines, etc.
Allergen immunotherapy (AIT) is increasingly being used to treat allergies. For example, in the treatment of asthma, allergen immunotherapy achieved remission 7 years after the end of treatment. But this area is just developing, so most people still have to live with the disease.
To live comfortably and safely, you need to follow simple rules and manage your allergies:
- avoid allergens or reduce contact with them as much as possible - for this you need to know the allergens exactly;
- Take medications only as prescribed by your doctor. Never self-medicate;
- If you have had anaphylaxis or are at risk of anaphylactic shock, always carry an epinephrine auto-injector with you - the only treatment for a severe allergic reaction;
- keep a diary in which you write down what you eat, what plants, animals, substances you come into contact with, what symptoms arise after contact;
- wear a medical bracelet in case you may have a severe allergic reaction. The bracelet should contain information about your illness and the necessary actions in case you are unable to speak.
Features when conducting a scarification test
• Before scratching, the skin is treated with 70% alcohol. • In children, the test is done on the upper back, in adults - on the shoulder. • Scratches are made on the treated area of the skin at a distance of no more than 5 cm. If the test is not carried out correctly (scratches are displaced), the result will be inaccurate. • Allergens are applied in the form of an extract or solution using a sterile needle or lancet. A separate needle is used for each stimulus. • The patient's hand should be motionless for 15 minutes. This is necessary so that the drops of irritants do not spread and the result becomes reliable. • Based on the reaction on the skin where the scratch was made, a conclusion is made as to how dangerous the substance is for a person in a particular case. Papules, redness, itching, swelling are a negative reaction to the components. • The result will be noticeable within 15 minutes. Upon completion of the measurements, the remaining drops of irritant are removed from the scratches. Up to 20 allergens can be applied in one test.
Attention!
A prerequisite for correct diagnosis is the absence of accompanying complications after the procedure - this depends on the highly qualified personnel, experience, diplomas and certificates confirming the right to perform research.
Results of the diagnostics
Patch testing is carried out during the diagnosis of contact and drug allergies. A patch impregnated with the allergen is applied. The prick test is similar to a prick test: the skin is punctured with a needle containing an allergen. Subcutaneous test is a test during which an injection of an allergen solution is injected under the skin. A skin test is a study that allows you to identify possible dangerous substances individually for the patient: • A positive, sharp result - very bright redness, the appearance of a large papule. • Positive result – redness is clearly visible, papule size 5 mm. • Weak positive result – with slight redness, a barely noticeable papule is formed. • Inaccurate reaction – there is no papule, only redness appears. In this case, a blood test is prescribed for comparison. • Negative result – no reactions on the skin appeared.