Intraoral air abrasive treatment: methods, devices, application possibilities
According to the Glossary of Terms in Prosthetic Dentistry, air abrasion is the process of treating the surface of a material through the use of abrasive particles driven by pressure from air or other gases. The second name for this method is sandblasting. In dental laboratories, sandblasting machines are used to clean materials and residues from the milling process, increase the roughness of the internal surface of crowns, and for a number of other practical purposes. In a clinical setting, air abrasion is provided by the simultaneous supply of abrasive particles and a water jet, which allows you to control their direction. Based on clinical need, there are several types of abrasive particles that differ slightly in their effect.
In this article, we will describe the instruments available on the market for performing air abrasive treatment, review the evidence regarding the feasibility of this procedure, and also analyze clinical protocols for using the method in dental practice. Air abrasive treatment, among other things, is also a tool for professional oral hygiene, however, in this article we will look at the specific capabilities of this method in orthopedic dentistry.
Devices for air-abrasive processing
At the moment, there are several devices available on the market for air abrasive processing that do not require the additional use of a water jet. These devices include MicroEtcher IIA (Danville Materials/Zest Dental Solutions) and EtchMaster (Groman Dental). These systems are effective for roughening and cleaning, although they also have a high level of contamination of both doctor's and patient's clothing during use. To minimize this effect, it is best to use devices with an additional water flow. Representatives of these are PrepStart H2O (Danville Materials / Zest Dental Solutions), AquaCare (Velopex), RONDOflex plus 360 (KaVo Kerr), Bioclear Blaster (Bioclear).
The effectiveness of such devices depends on the particle mixing mechanism, air pressure, and the level of particle and water flux density. For example, in some devices the mixing of particles occurs due to the formation of a vortex chamber inside the apparatus, while others provide mixing due to the vibration effect. In addition, some air abrasive systems are completely self-contained, while others can be connected to a dental unit. During the analysis of the literature, the authors of this article were unable to find publications concerning the comparison of the effectiveness of air abrasion procedures that did and did not provide for the additional use of water flow. It should be understood that the main purpose of the water flow is only to control the level of particle distribution.
Standalone devices
The advantage of a self-contained device is its pronounced functional flexibility and the ability to adjust parameters such as air pressure, particle flow rate and water flow rate. Two widely used models of these devices, PrepStart H2O and AquaCare, contain a reservoir for storing abrasive particles and liquid, and require only an air flow to operate. Both of these devices are activated by pressing a foot pedal. These devices differ only in that the design of the first assumes the presence of only one reservoir, which can be filled with different types of abrasive particles, while the design of the second is characterized by the presence of several such reservoirs, which can simultaneously contain several types of abrasive substances. In terms of infection control, these devices have removable tips that can be sterilized in an autoclave. PrepStart H2O uses a water reservoir that is filled by the user, so the hoses must be rinsed with a disinfectant solution at the end of each day. The water supply in the AquaCare device is carried out in parallel with a special liquid containing ethanol, therefore, the hoses are disinfected directly during operation.
Devices connected to the dental unit
Devices that connect to the dental unit have the advantage that they require less space in the dental office and do not impede the clinician's movement during a clinical appointment. Examples of such devices are RONDOflex plus 360 and Bioclear Blaster. These devices are equipped with reservoirs for filling them with abrasive particles, and air and water flows come from the dental unit. Also, these devices have removable tips that can be autoclaved, or they are autoclavable in their entire configuration.
Abrasive particles
To carry out the air abrasive treatment procedure, you can use several types of abrasive particles, which differ in their level of abrasiveness. Aluminum oxide is the most common agent used for these purposes, but other particles with a slightly lower level of abrasiveness can also be used, with which, for example, you can remove biofilm on the surface of a tooth.
Aluminium oxide
Aluminum oxide is a ceramic particle that is the most abrasive agent used in intraoral air abrasion procedures. These particles are characterized by an irregular shape with the presence of uneven edges, which ensures their abrasiveness. The density of aluminum oxide is 3.95 g/cm2. The average diameter of these varies from 30 microns to 90 microns, with larger particles being more abrasive. This type of abrasive agent is used to prepare the tooth, reduce hard tissue, and remove unwanted contaminants. In addition, aluminum oxide particles can achieve rougher surface finishes on certain dental materials such as metals, ceramics and composites.
Glass
Various glass particle shapes have also been extensively studied for their potential use in air abrasive machining processes. Glass particles are characterized by a spherical shape and lower density compared to aluminum oxide particles. The average particle size ranges from 50 µm to 90 µm. Considering the lower level of abrasiveness of glass particles, they are completely safe for tooth enamel and dentin. Therefore, these particles are more often used for surface cleaning purposes in which the level of surface damage should be minimized, for example, to remove excess cement or plaque. In addition, glass particles can also be used to clean metal tools. Bioactive glass particles have also been studied for their antibacterial properties and remineralization potential. In addition, these agents are used to obstruct dentinal tubules to minimize existing hypersensitivity symptoms.
Particles for cleaning
There are several types of abrasives intended solely for hygienic cleaning purposes, such as sodium bicarbonate, glycine, sodium calcium phosphosilicate, calcium carbonate and aluminum trihydroxide. Laboratory studies have demonstrated that the abrasiveness of all of these particles, with the exception of glycine, is high enough to modify the surface of a polymerized composite or glass ionomer. But despite this, these particles are ideal for removing plaque before starting restoration.
Evidence of the effect of air abrasion on bonding bonding
Data on the effect of air abrasive treatment on the strength of the bonding bond with enamel and dentin are very contradictory. This effect may be caused by the fact that the results of the tests performed depend on the type of adhesive used and the protocols for its application.
Previous studies
Studies examining the shear strength of bonding bonds during air abrasive machining provide partially conflicting results. Thus, Mujdeci and Goka reported that air abrasion (with 25 µm alumina particles at 120 psi) increased bond strength to enamel and dentin in total etch protocols. Souza-Zaroni et al reported a similar effect of alumina particles (27.5 µm at 60 psi) on enamel bond strength using self-etch bonding systems, but a similar result was not reported in adhesive assays requiring carrying out preliminary etching and washing off the etching agent.
On the other hand, Nikaido et al found that air abrasive blasting (at 41.8 psi) with 50 µm diameter glass beads significantly reduced the adhesive bond strength to enamel and dentin (using systems implying a preliminary etching stage), and aluminum oxide particles with a pore diameter of 50 microns reduce the strength of the bonding bond with the enamel, without affecting the strength of the connection with dentin. The results of scanning electron microscopy suggest a potential weakening of the tooth structure after air abrasive treatment, which may consequently reduce the strength of the adhesive bond. Roeder et al reported that when air abrasion (120 psi aluminum oxide) was used instead of a phosphoric acid etchant, the level of bonding force to enamel and dentin was significantly reduced. Some studies indicate the absence of any effect on the bond strength between the composite and tooth structures after air abrasion. Thus, Los and Barkmeier found no effect on the bond of self-etching bond to dentin when pretreating the tooth surface with 50 µm aluminum oxide particles at 60 psi. inch or hydroxyapatite particles ranging in size from 20 to 40 microns. Similar results were also noted by Roeder et al regarding 27- and 50-μm alumina particles at 120 psi. inch.
Laboratory research
During the preparation of this review, a laboratory study was also conducted to study the effect of air abrasion on the bonding strength of enamel (pre-etched) and dentin (pre-etched and self-etched systems). After institutional approval was obtained, the extracted teeth were segmented to form flat enamel (n = 20) and dentin (n = 40) surfaces, which were then polished with silicone tips. Half of the test specimens (enamel n = 10, dentin n = 20) were treated with PrepStart H2O for 10 seconds with 50 µm alumina particles (Danville Materials/Zest Dental Solutions) at 60 psi and then they were washed. All enamel samples (n = 20) were etched with 37% phosphoric acid (Scotchbond Universal Etchant, 3M Oral Care) for 30 seconds. Some dentin samples were also etched (n = 20) with 37% phosphoric acid for 15 seconds before applying the adhesive, and some (n = 20) were treated with a self-etching bond without prior etching. All samples etched with orthophosphoric acid were washed for 10 seconds under running air and water.
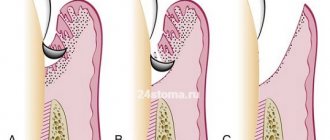
All samples were coated with the same adhesive (Prelude One, Danville Materials / Zest Dental Solutions), which was then cured with a lamp (Elipar S10, 3M) with an output power of > 800 mW/cm2. A 2.35 mm diameter cylindrical composite sample (Prestige, Danville Materials/Zest Dental Solutions) was applied to the machined surfaces of the samples and cured for 20 seconds. Specimens were kept moist at 37°C for 24 hours and then thermally cycled (5ºC and 55ºC, 15 second dwell time, 10,000 cycles) after which they were subjected to shear loading to bond failure using a specially designed universal testing apparatus (Instron 5565, Instron ). Finally, the samples were examined using scanning electron microscopy (SEM). The T-test revealed no difference in bond strength between enamel air abrasion and non-air abrasion treatments (P = 0.437), and one-way ANOVA confirmed similar results for dentin (P = 0.515). Thus, when processing enamel, the bond strength was 28.4 ± 6.7 MPa, and without it - 30.4 ± 4.5 MPa. As for dentin, in cases of etching and abrasive treatment, the strength of the adhesive connection reached 27.3 ± 5.2 MPa, and without it - 24.9 ± 9.8 MPa, and in cases of using a self-etching agent with air abrasion - 22. 8±7.2 MPa, and without it - 28.9±3.6 MPa. SEM results showed that the structure of dentin enamel becomes rougher after air abrasion treatment, and the texture remains specific even after etching with phosphoric acid (photos 1-10). But despite the higher roughness, it had virtually no effect on the value of the adhesive bond, determined by the shear force parameter. One can only assume that adhesion in cases of using self-etching bonds becomes only slightly stronger, which was also found in studies by de Souza-Zaroni and colleagues.
Photo 1. View of the enamel sample before etching and air abrasive treatment.
Photo 2. View of an enamel sample after air abrasive treatment before etching.
Photo 3. View of the enamel sample after etching without air abrasive treatment.
Photo 4. View of the enamel sample after etching and air abrasive treatment.
Photo 5. View of the enamel sample after etching and air abrasive treatment at a higher magnification.
Photo 6. View of a dentin sample before etching and air abrasive treatment.
Photo 7. View of a dentin sample before etching and air abrasive treatment.
Photo 8. View of a dentin sample after etching without air abrasive treatment.
Photo 9. View of a dentin sample after etching and air abrasive treatment.
Photo 10. View of a dentin sample after etching and air abrasive treatment at higher magnification.
Clinical Applications
Cavity preparation
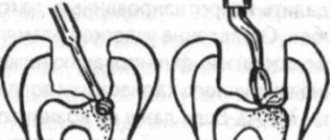
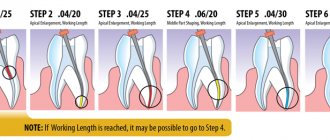
The clinical benefits of cavity preparation by air abrasion are that it provides a more conservative approach to hard tissue reduction. Several studies have examined the ability of abrasive particles to selectively remove carious dentin without affecting healthy tooth tissue, but this has proven to be nonspecific. One study even reported that aluminum oxide particles removed healthy dentin and enamel tissue to a greater extent than caries-affected tissue. Of course, the air-abrasive preparation method takes longer than preparation using boron, but the effectiveness of this process is influenced by a number of parameters. First, the "cutting" power of air abrasion is dependent on air pressure: the current recommended pressure level for preparation is 100 psi. Particle flow rate can also affect preparation efficiency, but must be adjusted based on air pressure. If the particle flow rate increases without sufficient air pressure, the volume of particles will not move enough and the additional particles will only cause more dust volume. Ensuring that there is a sufficient amount of abrasive particles in the device's accumulator before and during preparation is also extremely important as this directly affects the particle flow rate. Finally, the angle at which the working part of the nozzle is directed relative to the surface of the tooth, and the distance to the tooth, also determine the effectiveness of the preparation. Positioning the nozzle at an angle of 60 degrees to the surface allows for effective V-shaped tissue reduction at a distance to the tooth of up to 5 mm. But one of the main advantages of air abrasive preparation is patient comfort, especially in cases where anesthesia was not used.
Cleaning after preparation
Air abrasive blasting can also be used to further clean teeth after preparation and before adhesive application. This approach allows you to remove the remains of previous fillings, discoloration and temporary cement (photo 11-14). In addition, the abrasive particles allow the internal surfaces of the stump to be smoothed, resulting in better adaptation of the material used for restoration (photo 15-16). Considering that the adhesion phenomenon is extremely sensitive to surface cleanliness, it can be assumed that from this point of view, air abrasion still accompanies the achievement of more effective results of dental treatment.
Photo 11. Air abrasive treatment of enamel.
Photo 12. View of the enamel surface after air-abrasive treatment before etching.
Photo 13. View before air abrasive treatment.
Photo 14. View after air abrasive treatment.
Photo 15. View of cavities before air abrasive treatment.
Photo 16. View of cavities after air abrasive treatment.
Biofilm removal
Aluminum trihydroxide air abrasive can be used to remove plaque, minor tartar, overhanging enamel margins, defective restorations and linings, and for specific soft tissue retraction. Removing biofilm also improves bond strength and minimizes the subsequent effect of microleakage. Given the difficulties with visualizing biofilm, it is recommended to use different dyes to identify it, which should be applied several times (photo 17-19). Considering that abrasive particles, with the exception of glycine and sodium bicarbonate, can alter the enamel surface, re-application of coloring agents after air abrasion should be avoided, as they can cause discoloration.
Photo 17. Visualization of plaque using dye.
Photo 18. Air abrasion with aluminum trihydroxide to remove biofilm.
Photo 19. View after air abrasive treatment.
Summary
Air abrasive treatment is one of the methods of tooth preparation, as well as an additional method for increasing the predictability of the functioning of composite restorations. Although there is conflicting evidence for improved bonding following air abrasion, this method at least allows for cleanup of the tooth surface after preparation and also avoids the need for anesthesia in some cases. When using the capabilities of air abrasion, the parameters of the device used should be optimized to achieve the required results of the intervention.
Authors: Chan-Te Huang, DDS Jihyon Kim, DDS Celin Arce, DDS, MS Nathaniel C. Lawson, DMD, PhD
How is the procedure performed?
The process takes place under the strict supervision of a dentist. The first step is professional cleaning - plaque is removed from the enamel. Only after cleaning is completed can polishing begin.
The whole procedure takes no more than 40 minutes. The session is performed without anesthesia. The choice of nozzle is of great importance. It is selected based on an assessment of the current condition of the tooth and the level of sensitivity.
During grinding, a specially selected paste is used. It is applied to a holder connected to the device.
The part with the paste applied to it begins to rotate at high speeds - in some cases they can reach up to five thousand per second.
There is no need to worry about the possibility of damage to the enamel, because a professional dentist will not allow this to happen.
Main indications and contraindications for the procedure
The main indication for performing the process is the roughness of the enamel. It can appear due to the individual characteristics of the body, as well as after professional cleaning.
At the first free consultation, the dentist will check the condition of the oral cavity for the presence of major contraindications.
These include:
- High sensitivity and severe bleeding of the gums.
- Aggravated periodontitis.
- Caries, especially with deep damage to the tooth tissue.
- Individual increased sensitivity of enamel.
You should not carry out polishing even if there are pockets of inflammation in the oral cavity. In this case, it will be necessary to first carry out treatment and eliminate them.
What will be required after the procedure
The recovery process itself takes little time. Many patients experience increased sensitivity during the first 24 hours after visiting the dentist. For this reason, it is worth limiting the consumption of food that is too hot or cold.
For two or three days, you should also give up drinks and foods that can strongly stain the enamel. These include tea, coffee, some types of vegetables, fruits and berries.
At the Novodent clinic in Khimki, our doctors will perform all the necessary operations, both cleaning and subsequent grinding of the enamel.
We use high-quality compounds and proven tools, the appointments are conducted by experienced dentists - this guarantees that there will be no damage to the enamel during the process and the result will be exactly what you expected.
To schedule your first free consultation, call or submit a request on the website. We guarantee the quality of the result and offer affordable prices.