Enamel hypoplasia is a non-carious lesion of teeth that occurs before tooth eruption during the development of its tissues. The term “enamel hypoplasia” is conditional, since changes are also observed in other tooth tissues - dentin and pulp.
Terminology of dental enamel hypoplasia
Dental enamel hypoplasia is a qualitative and quantitative violation of tooth enamel. This definition of the disease is most often found in Russian-language literature. In international sources, enamel hypoplasia (including prenatal and neonatal) refers only to its quantitative changes - thinning, pits, grooves. Qualitative changes (changes in color, transparency) in foreign literature are opacity, hypomineralization, dismineralization and non-endemic mottling of enamel (ICD-C).
Enamel hypoplasia in children
Enamel hypoplasia in children can develop in utero, during the newborn period, before and after the first year of life, up to the age of three. Despite the period of its occurrence, the mechanism for the appearance of changes in enamel is the same. Initially, the function of ameloblasts during the formation or secretion of enamel substance is reduced or impaired. As a result, the construction of the enamel protein matrix and its mineralization are damaged. In the later and most severe stages of the disease, vacuolar changes in ameloblasts and their destruction are detected. The cells can no longer function and amelogenesis stops.
Degrees of the disease
The appearance of dark spots on the teeth is one of the signs of hypoplasia.
There are 3 degrees of development of Hutchinson’s teeth, which differ in shape and complexity:
- The initial stage of hypoplasia - small dark spots of pigmentation on the enamel layer of some or all teeth
- Moderate degree of the disease - the surface of the enamel layer is covered with convex or concave grooves and depressions. At the same time, Hutchinson's triad may begin to appear
- A severe degree of hypoplasia is characterized by abrasion of enamel or visible deformation of dental units
Therapy is necessary for any of the degrees described, but its methods will vary at each stage.
Causes of enamel hypoplasia
There are several groups of causes of enamel hypoplasia. Depending on the period of their exposure, temporary or permanent teeth are affected.
Enamel hypoplasia of primary teeth
In the occurrence of enamel hypoplasia of primary teeth, the key etiological factors are:
- Causes of prenatal hypoplasia (the main period of exposure to a negative factor is pregnancy):
- Maternal diseases: hormonal disorders, epilepsy, rubella, toxoplasmosis, alcoholism;
- Physical factors (irradiation);
- Insufficient intake of vitamins, micro- and macroelements from food.
- The causes of neonatal hypoplasia (in the neonatal period - the first 56 days of a child’s life) can be prematurity, birth trauma, asphyxia, hemolytic disease of the newborn.
Enamel hypoplasia of permanent teeth
Hypoplasia of the enamel of permanent teeth is most often associated with diseases of the child that disrupt the metabolism in the body.
These are diseases:
1) Central nervous system: the mineral metabolism of phosphorus and calcium is disrupted, the amount of magnesium and potassium in the blood and bones decreases;
2) Endocrine system:
- Hyperthyroidism promotes the supply of calcium and phosphorus to the teeth and bones. With hypothyroidism, these elements are washed out.
- Against the background of insufficiency of the parathyroid glands, the content of calcium and phosphorus in the blood increases, decreases in the bones, nails, hair, and the lens are also affected;
3) Toxic dyspepsia and other diseases of the digestive system (due to insufficient absorption of calcium and phosphorus);
4) Hypovitaminosis C, D, E (up to rickets);
5) Acute infectious diseases;
6) Allergic diseases;
7) Insufficient nutrition.
Also, the quality of the enamel of permanent teeth depends on the condition of their temporary predecessors. Chronic apical periodontitis, mechanical trauma and removal of primary teeth with trauma to the follicle of a permanent tooth can lead to its hypoplasia.
Dystrophies (stigmas)
The occurrence of a number of dystrophies in congenital syphilis is not associated with exposure to Treponema pallidum (the causative agent of syphilis) and does not have any diagnostic value. They develop with many infectious diseases and intoxications, for example, with parental alcoholism. Stigmas can indicate that a child may be affected by syphilis and help in making a diagnosis.
Rice. 16. Enlarged and protruding frontal and parietal tubercles without a dividing groove (“Olympic forehead”). The anomaly occurs in 36% of patients.
Rice. 17. A high hard palate (“lancet” or “Gothic”) occurs in 7% of cases.
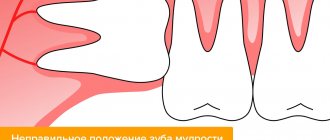
Rice. 18. Diastema (distance, gap) between the central incisors. Most often found on the upper jaw.
Rice. 19. A thickened sternal end (usually the right) of the clavicle (Ausitidian-Igumenakis symptom) occurs in patients with congenital syphilis in 25% of cases. The cause of the pathology is hyperostosis. In 13 - 20% of cases with congenital syphilis, there is an absence of the xiphoid process (Queir's axiphodia).
Rice. 20. A shortened (infantile) little finger (Dubois symptom) is recorded in 12% of cases with congenital syphilis. The little finger may be curved and turned towards the other fingers (Hissar's symptom).
Rice. 21. Stigmas indicating congenital syphilis may include spider fingers—abnormally long and narrow fingers (arachnodactyly).
Rice. 22. Girls and boys with congenital syphilis may experience hypertrichosis - growth of hair on the forehead (Tarkovsky hypertrichosis).
Classifications of enamel hypoplasia
The most common classification of enamel hypoplasia is the classification of M.I. Groshikov. It is based on different etiologies and the number of teeth affected. Based on this, methods of treatment and prevention of various forms of hypoplasia differ.
Systemic enamel hypoplasia
Systemic enamel hypoplasia is a disorder in the structure of all teeth, but more often in groups associated with close periods of formation and eruption.
Such diseases in the ICD-C (1995) as prenatal enamel hypoplasia, neonatal enamel hypoplasia, enamel hypoplasia, non-endemic mottling are nothing more than “systemic enamel hypoplasia” according to M.I. Groshikov.
Features of the clinical manifestation of defects in systemic enamel hypoplasia:
- appearance from the moment of eruption;
- symmetrical, of the same size on teeth of the same name;
- localized parallel to the chewing surface or cutting edge, most often on the tubercles or vestibular surface.
There is also a relationship between the defect and the action of the damaging factor:
- The type of defect (qualitative or quantitative change in enamel) depends on the intensity of the factor;
- Localization of the defect - depending on the time of its exposure;
- The width of the defect depends on the duration;
- The number of defects indicates the frequency of action of the damaging factor.
Read also
How to place veneers
The installation of veneers is performed for the purpose of aesthetic restoration of the dentition.
How long do you wear braces and what affects the timing?
When deciding on the use of orthodontic structures, patients are often interested in how long they wear braces on their teeth.
Forms of enamel hypoplasia
Clinically, the following forms of enamel hypoplasia are distinguished: spotted, cup-shaped (erosive), grooved (wavy) forms, thinning or aplasia of the enamel.
The spotted form is spots and stripes, most often white or yellow, with clear or fuzzy contours. Their surface can be smooth and shiny or rough and dull. Shiny smooth enamel means demineralization of its subsurface layer, dull and rough – changes in the surface layer at the end of the enamel formation process.
Cup-shaped, grooved forms, thinning, aplasia of enamel are manifested by areas of hypoplasia through which dentin is visible, grooves, aplasia (complete absence) of enamel. The edges, walls and bottom of the defects are sometimes yellow-brown pigmented and smooth.
Separately, it is necessary to mention molar-incisal hypomineralization. Its characteristic feature is damage to one to four permanent molars, often combined with damage to the incisors. Clinically, these are cloudy spots of white, yellow or brown color, sometimes covering the entire crown of the tooth. Children may be bothered by teeth chipping and sensitivity. Because of this, they may refuse to brush their teeth, which soon leads to the development of caries. Parents may be concerned about the unaesthetic appearance of their teeth.
Teeth of Hutchinson, Fournier and Pflueger
Also manifestations of systemic enamel hypoplasia are the teeth of Hutchinson, Fournier and Pfluger. They are characterized by a change in tooth shape. The main reason is late congenital syphilis.
Local enamel hypoplasia
Local enamel hypoplasia (Turner's tooth) is a violation of the development of enamel (sometimes dentin) of individual permanent teeth. As a result, the tooth changes color: it becomes white or yellow-brown, and areas of hypoplasia appear on it. Turner's tooth is directly related to the periapical inflammatory process of the primary tooth.
Focal enamel hypoplasia
With focal enamel hypoplasia (regional odontodysplasia), underdevelopment of all dental tissues is observed. Typically, the process involves several teeth located nearby. These temporary, and subsequently permanent, teeth are characterized by late development and eruption. After eruption, the teeth are yellowish, with a rough surface. The characteristic name for such teeth is “ghost teeth,” which is also due to their special appearance on an x-ray. The enamel and dentin are thin, their density is reduced, the pulp chamber is large, the roots are wide and short, with open apexes.
Other signs of late congenital syphilis
Lesions of the skeletal system
Osteoperiostitis and periostitis, gummous osteomyelitis and osteosclerosis are the main types of bone lesions, which occur in 40 - 50% of congenital syphilis. The lower legs (59%), nasal bones (18%), forearms (10%), skull bones (5%), and hard palate (4%) are affected.
Lesions of internal organs
Pathology of internal organs with congenital syphilis is registered in 20 - 25% of cases. The liver, spleen and kidneys are most often affected. With syphilitic damage to the heart, all its membranes, valves and vessels are affected. There is dysfunction of the thyroid, pancreas, thymus and gonads, pituitary gland and adrenal glands.
Nervous system lesions
Pathology of the nervous system with congenital syphilis occurs in 27 - 43% of cases. Of these, more than 50% are caused by damage to the brain, 32% to the spinal cord, and 11% to the tabes dorsalis. In 23% of cases, mental disability develops. With congenital syphilis, mental retardation, speech disorder, hemiplegia and hemiparesis, tabes dorsalis, and Jacksonian epilepsy are recorded. The child constantly suffers from headaches. Secondary atrophy of the optic nerves develops.
Syphilitic chorioretinitis
Syphilitic chorioretinitis leads to changes in the retina and choroid of the eye. Visual acuity is not reduced. Optic nerve atrophy leads to vision loss. With syphilis in children, a combination of chorioretinitis and damage to the optic nerve is more common.
Rice. 23. The photo shows chorioretinitis in early congenital syphilis. The disease is characterized by the “salt and pepper” symptom, which is characterized by the appearance of lumps of pigment and zones of depigmentation along the periphery of the fundus.
Treatment of enamel hypoplasia
Several methods are used to treat enamel hypoplasia. The choice of each depends on the violation of aesthetics, type, depth, area of the defect, degree of enamel mineralization, motivation of the child and parents, and technical capabilities.
The essence of the conservative method is to increase the mineralization of hard tooth tissues. This is both endogenous and exogenous use of vitamins, preparations containing fluorine, calcium, phosphorus. It can be used both independently and as an initial step before other methods.
Microabrasion and/or bleaching is carried out after the mineralization of the tooth is completed. The technique consists of etching the enamel, followed by grinding it with a minimally abrasive bur and polishing it with a rubber cup. This method is effective if the defect is in the surface layer of the enamel or when it is clouded.
The surgical method is preparation and then filling. It is also carried out either after conservative therapy or after mineralization of the tooth is completed. Used for the deepest defects in the enamel. Options include filling with GIC (followed by replacement with composite), composite materials, veneers, laminates and crowns.
Another treatment tactic for focal hypoplasia. The optimal approaches to restoring teeth in this case are covering the teeth with crowns soon after eruption or removing them with prosthetics.
Prevention of enamel hypoplasia
The main directions of prevention of enamel hypoplasia:
- Prevention of diseases in a pregnant woman, her balanced diet;
- Prevention and treatment of somatic diseases in young children;
- Sanitary and educational activities of a dentist in a antenatal clinic, a children's clinic;
- Treatment or removal of temporary teeth with complicated caries;
- Prevention of trauma to temporary teeth;
- Atraumatic removal of a temporary tooth.
The article was written by Titenkova O.V. especially for the OHI-S.COM website. Please, when copying material, do not forget to provide a link to the current page.
What is a gap from a dental point of view?
In dentists' language, the gap between teeth is called diastema (from Greek - “gap, distance”). According to statistics, varying degrees of this defect are present in every fifth adult on the planet. In childhood, increased interdental space is often temporary; it is observed in 50% of preschool children. Diastema refers to an abnormally large empty space between the incisors (can reach 10 mm).
Patients often confuse a diastema (a gap between “units”) with a trema (a gap between any teeth in a row), although formally these are completely different defects, although similar in essence. Accordingly, the approach to treatment/elimination is different in both cases.
Reviews
If a child is found to have Turner teeth, his parents have no reason to panic. This is a relatively mild form of hypoplasia that can be corrected with appropriate treatment.
If your child has been diagnosed with MGE, please share your personal experience with us. How severe was the destruction of the enamel, what treatment method was used, what was the result? The feedback form is at the bottom of this page.
If you find an error, please select a piece of text and press Ctrl+Enter.
Tags: enamel destruction
Did you like the article? stay tuned
Previous article
How effective are braces for diastema and are they always necessary?
Next article
What filling materials are used in pediatric dentistry?
Tips for parents
Many parents do not even suspect that dental hypoplasia is a very common disease among children. In order to alleviate the child’s condition, the following actions must be taken:
- Eliminate all sour and sweet foods from your diet.
- Use special toothpastes.
- For small children, purchase silicone finger brushes for oral hygiene.
- Carry out the procedure of silvering your teeth regularly.
- Monitor their condition and promptly fill teeth if necessary.
Diagnostics
Patients with aplasia usually come to the dental clinic with complaints of increased tooth sensitivity. During the examination, the cause of this phenomenon is revealed.
With hypoplasia there may be no complaints. If the defects are minor, they are usually an accidental discovery. But in most cases, parents pay attention to stains on the child’s enamel and make an appointment with a dentist.
To carry out an accurate diagnosis, the doctor needs to collect an anamnesis, obtain detailed information about how the pregnancy proceeded, how the child developed in the first year of life. Studying medical records will provide detailed information about past illnesses. It is important for the dentist to know when defects appeared on the teeth. If the patient is a school-age child, the specialist will clarify whether a similar problem occurred on baby teeth. The dentist will also ask if this phenomenon has occurred among close relatives; perhaps the damage to the enamel is hereditary.
After the conversation, the dentist proceeds to examine the oral cavity. This makes it possible to establish the size, prevalence and nature of the defects, as well as to carry out a differential diagnosis with other lesions, such as caries.
Prevention
To prevent enamel hypoplasia from developing in an adult, preventive measures are necessary. These are quite simple rules, following which you can completely avoid the disease. But you will have to pay attention to prevention in advance.
Nutrition
Proper diet and hygiene are the essence of preventing hypoplasia
A large role in the prevention of hypoplasia is given to proper, nutritious nutrition. A woman should pay close attention to her diet, starting from the planning stage of pregnancy. It is necessary to ensure that the child eats fully and correctly. After switching to complementary feeding, instead of breast milk or formula, the baby’s diet must include:
- Products containing fluorine and calcium (cottage cheese, milk, cheese and others);
- Vitamin D in the form of a ready-made preparation or exposure to the sun for a sufficient time;
- Products containing vitamin C (oranges, tangerines, broccoli, spinach, cranberries);
- Foods containing vitamins A and B - seafood, legumes, carrots, poultry.
Hygiene
From the age of one, your baby should begin to be taught daily oral hygiene. At first, it may just be a game, morning and evening, especially if the baby doesn’t like brushing his teeth at all. Here parents will need imagination, and, of course, they need to set a personal example. You need to teach your child to rinse his mouth after every meal. It is necessary to visit the dental office twice a year in order to identify problems at an early stage.