Diastema is an enlarged interdental space separating the central incisors of the upper or lower jaw. The gap can be 1-6 mm or more, and even if small, it affects the aesthetics of the smile and attracts attention. An unpleasant consequence of the appearance of a diastema is not only unaesthetics, such a defect affects the quality of speech and causes difficulties in communication.
It is worth noting that diastema is often accompanied by other anomalies in the position and shape of the teeth. Therefore, it is important to take a comprehensive approach to diagnosing and eliminating the defect.
Causes of diastema
The most common cause of diastema is genetic predisposition. Anomalies of the frenulum play a significant role - a short or massive frenulum of the upper lip or its low attachment. Hereditary predisposition is determined by the genetic characteristics of the structure of the dental system and oral tissues. There are also less common reasons:
- the presence of supernumerary impacted dental units - such teeth literally push the front incisors apart, preventing them from closing tightly;
- microdentia - incisor teeth are too small;
- partial edentia - the loss of any tooth in a row can cause the rest to shift;
- late eruption of permanent teeth - defects in the structure of the jaws, discrepancy between their sizes and teeth;
- jaw tumors;
- alveolar cleft;
- bad habits - prolonged sucking of pacifiers, the habit of biting nails, biting pens/pencils, gnawing seeds, etc.
Ask a Question
Indications for installation
It is worth noting that aligners are recommended only if the clinical picture allows us to determine the pathology as mild or moderately severe. At later stages of development, the pressure exerted by the polymer structure becomes insufficient for displacement, which necessitates the installation of braces or a full-fledged operation.
The list of pathologies that can be eliminated with the help of aligners includes:
- Anomalies of the dentition - rotation, crowding, the presence of deviated units;
- Incorrect development of the bite, characterized by a shift in the midline and a violation of the occlusal closure;
- Insufficiency of the dental arch, requiring narrowing or expansion;
- Interdental gaps that disrupt aesthetics and contribute to the accumulation of infection.
In addition, the use of aligners is recommended if there are factors that limit other methods - for example, an allergy to medical steel, or insufficiency of bone tissue that precludes dental prosthetics.
Types of diastemas
There are true and false diastema. False teeth occur during the period when baby teeth are replaced by permanent teeth. Such a diastema is normal in children - the jaw grows, which explains the appearance of gaps between the upper and lower teeth. By the time the bite change is completed, this feature disappears. True diastema occurs in the permanent dentition and does not disappear on its own, only with dental care.
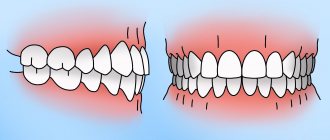
There are symmetrical and asymmetrical diastemas. In the first case, the incisors are displaced at the same distance, and in the second, one of the teeth is positioned normally, while the other is displaced.
The problem can be aggravated not only by the presence of a gap, but also by rotation of the teeth along the axis, moving forward or, conversely, inside the oral cavity.
Mini-implants - as a basis for orthodontic treatment
The procedure for installing mini-implants is carried out under local anesthesia and does not require any incisions or sutures. A puncture is simply made in the tissue through which the surgeon implants a titanium implant. But simple and low-traumatic manipulations should be performed by a highly qualified specialist who can take into account the peculiarities of the location of the dental roots so as not to injure the tooth.
- In this example, small orthodontic dental implants will be installed next to the lowered upper “seven” - one each on the vestibular (external) and lingual (internal) sides.
- The orthodontist will glue special hooks to the molar on both sides, which will be connected to the heads of the implants using elastics. This way, the doctor will create a constant force, supported by the implants, pulling the sagging tooth back into the jaw bone.
- As with treatment with braces, stretchable elastic bands will need to be replaced periodically, for which you will have to visit the clinic. At the same time, the orthodontist will monitor the process, correcting the movement of the problem tooth.
As a result, a place for prosthetics will be obtained without removing, depulping or grinding the molar.
Symptoms of diastema
The gap between the teeth can have different severity. The gap is rarely narrow and parallel; more often the central incisors have a deviation, so the gap is characterized by a triangular shape. The apex of such a triangle can be facing both the gums and the cutting edge of the teeth. The diastema is often accompanied by a powerful frenulum of the upper lip, part of which is attached to the crest of the alveolar process and the incisive papilla. The defect is accompanied by other anomalies. The most common of them are the following:
- Trema - lack of close contact between the teeth, gaps not only between the front incisors, but also the chewing teeth;
- microdentia - small teeth;
- malocclusion;
- rotation of the cutters along the axis.
This exacerbates the aesthetic problem. A person may experience embarrassment and discomfort when talking, smiling, and avoid new acquaintances and communication.
Diastema increases the risk of developing periodontal disease in the area of the front teeth. This is due to improper distribution of the chewing load, unstable position of the teeth - lack of lateral supports. Periodontal disease can cause healthy teeth to become loose and there is a high risk of losing them.
Very often the anomaly is accompanied by speech disorders. This is usually expressed in the inability to pronounce certain sounds, a lisp, and a characteristic whistling.
Manufacturing materials and treatment stages
When a patient applies, a preliminary examination is carried out to determine existing anomalies, determine the degree of their severity and negative impact on aesthetics and functionality, and also select a treatment method. Comprehensive diagnostics includes hardware examination (X-ray, CT, orthopantomogram) and accompanying tests necessary to exclude possible contraindications.
An impression taken from the jaw row, as well as indicators obtained during scanning, serve as the basis for creating a three-dimensional model on which each stage of the correction course is calculated. The doctor calculates the number of pairs of aligners needed to eliminate the identified defects and announces the cost of treatment in advance.
The duration of treatment using aligners depends on the complexity of the pathology - a period of 6-12 months is considered the standard range. Throughout the course, the patient must strictly adhere to the pair replacement schedule, and also regularly visit the clinic to monitor progress. The achieved result is fixed with the help of retainers - similar structures designed to prevent reverse displacement of the rotated fangs.
Diagnosis and elimination
The distance between the front teeth is noticeable to the naked eye. But diagnostics are necessary to find out the causes of the defect. The dentist examines the oral cavity and may prescribe the following examinations:
- targeted radiography;
- panoramic shot, or OPG;
- taking impressions and making a plaster model of the jaws.
The specialist will take into account the shape, size, position of the incisors, the structure and condition of the root system, examine the frenulum, determine the symmetry of the defect, the nature of the bite and other parameters. Only after this the doctor will suggest the optimal method for correcting the deficiency. Sometimes additional consultation with a dental surgeon, orthodontist, orthopedic dentist, or periodontist may be required.
Treatment of diastema may require the use of orthopedic, orthodontic, surgical methods, or a combination of these. There are several common schemes:
- Cosmetic restoration - installation of composite veneers.
- Orthopedic method. Installation of ceramic veneers or crowns: metal-ceramic, all-ceramic, etc. Restoration of dentition using implants with artificial crowns and other types of structures.
- Surgical method. Plastic surgery of the frenulum of the lips or tongue, removal of impacted, dystopic, supernumerary teeth.
- Orthodontic method. Installation of removable or fixed systems that allow you to change the position of teeth (plates, braces).
Cosmetic restoration is used for microdentia if the roots of the incisors are located correctly, and the problem arose due to the deformation of the crowns or their small size. Veneers can also be used for minor defects in the enamel of the incisors.
The orthopedic method is relevant when the interdental gap arises as a result of the absence of adjacent teeth. Also, installing artificial crowns will help with partial destruction of the incisors.
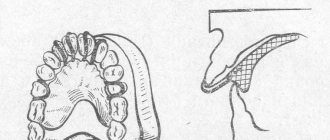
Plastic surgery of the frenulum is necessary when it is shortened or has a changed structure. Sometimes this method is combined with other methods. If orthodontic treatment is planned, the patient will first have the frenulum adjusted. After this, if the doctor deems it necessary, the installation of orthopedic structures will be prescribed.
Why do teeth shift?
The most common reason is a violation of the integrity of the dentition
. As a result, antagonist teeth cease to participate in the chewing process, and the load on other (working) teeth increases. The contact of the teeth (occlusion) is disrupted and becomes traumatic, destroying the ligaments and stretching the collagen fibers that hold the tooth. A tooth that does not have contact when the jaws are closed begins to move vertically. So, if the lateral upper teeth are missing, then the lower ones move vertically upward. And if there are no lower teeth, the upper ones are displaced. For large defects (6 or more missing teeth), the movement is strictly vertical. But almost every tooth has a main and secondary antagonist. They prevent the tooth from moving strictly vertically. With small defects (1-3 teeth), there is also a tilt towards the lost units. The displacement of teeth after extraction becomes more pronounced the longer prosthetics are delayed. Therefore, dentists recommend restoring the dentition without delay.
Other reasons:
- Caries of occlusal surfaces
(points of contact when closing the jaws)
The more the crown is destroyed, the less the tooth participates in the chewing process, up to its complete exclusion from it. Then the displacement mechanism develops according to the same pattern as with dentition defects.
- Increased enamel abrasion
A change in tooth height, even by one or two millimeters, changes the entire articulatory picture, disrupting the occlusion and leading to the same results as in the first two cases.
- Periodontal disease
The periodontium is a ligamentous-muscular apparatus that holds the tooth in its socket. With periodontitis, the ligaments weaken and cannot hold the teeth in their original position. They begin to stagger and “move apart” to the sides. A classic example of combined movement during periodontal inflammation is the fan-shaped discrepancy of the upper frontal teeth.
- Wisdom teeth
They begin to grow after the dentition has formed. An obstacle in the form of a neighboring tooth can stop growth, or turn the “eight” to the side. Abnormally located teeth are not in the bite and violate the occlusion. An impacted (unerupted) tooth can cause the front teeth to shift and become crowded.
- Wisdom teeth removal
One of the complications is tooth displacement after wisdom tooth removal. Extraction can disrupt the occlusion by moving the adjacent tooth, the “seven,” to the vacant space.
Why eliminate diastema
Some patients consider the diastema to be a peculiar highlight and do not think about how to remove the gap between the front teeth. However, aesthetic indications are not the only reason to see a doctor. Normally, the lateral surfaces of all teeth touch. This helps maintain a stable position of both individual teeth and the entire dentition - this way the teeth simply have nowhere to move. Diastema can cause changes in the position of other teeth and provoke the development of gum disease due to a violation of the distribution of chewing load.
A large gap between the incisors changes diction, and in case of serious problems with pronunciation, even after correction, the help of a speech therapist is often required. Therefore, it is important to deal with the defect as early as possible in order to prevent the development of complications.
At STOMA clinics you can get professional help in eliminating diastema. Our specialists perform plastic surgery of the lip and tongue frenulum, install veneers and select appropriate methods of bite correction. You can make an appointment for a consultation by calling the specified phone number or using a special form on the website.
Correction of misaligned teeth
What to do if you see, for example, how the teeth on the lower jaw have shifted?
It seems to many that it is no longer possible to correct the situation in adulthood - the teeth will still return to the wrong position, and besides, correcting the bite is long, difficult and unaesthetic. Fortunately, orthodontists today are successfully correcting misalignments in adult patients. To do this, they use 2 orthodontic systems, which, using the pressure of a calculated force, carefully move the teeth to the correct position.
- Braces
A classic non-removable system that consists of a metal arch, braces - elements that are fixed to each tooth, and locks or ligatures that secure the arch in the braces. Today, these systems have become much more compact and comfortable, and we are no longer talking about long years of correction, since the average treatment period is only 1.5–2 years. Doctors have metal, ceramic, sapphire and combined systems at their disposal. There are also lingual braces - they are fixed on the lingual side of the teeth and are not visible when you smile. - Aligners
A removable system of aligners developed about 3 years ago that are worn on the teeth. For each patient, based on photographs and impressions of the jaws, an individual set of aligners is created, which the patient himself changes according to a schedule drawn up by the orthodontist. Unlike braces, aligners can be removed for 2 hours a day to eat and brush your teeth.
However, in any case, after removing the orthodontic system and completing the bite correction, a period of retention follows - when the patient wears retainers that prevent the teeth from returning to their previous position.
Treatment tactics
There are five methods for correcting the disorder in question:
- Expansion of the tooth area with braces.
- Removal of a tooth.
- The use of elastic traction.
- Surgical method.
- Prosthetics and restoration.
Let's consider each of the treatment methods in detail.
Expansion of teeth with braces
Most often, the most complex displacement is expressed in the discrepancy between the center of the teeth of the upper and movable jaw.
In this case, the doctor’s task is to ensure that not only the center of the two rows coincides, but also that the jaw midline completely matches the line passing through the center of the face.
If there is a shortage of space in the jaw arches and there is an asymmetrical displacement, braces are used to expand the problem area on the top row on the right side.
At the same time, on a mobile jaw, the correction by the system occurs in the opposite way - the problem area on the left expands. According to this principle, treatment with a brace system will be successful and the depth of overlap of teeth in the frontal zone will be noticeably normalized.
Remarkable! In the treatment of the anomaly in question, classical brace designs are capable of showing good results.
The video presents tactics for treating anomalies using combined braces.
Removal of a tooth
When the midline of one of the arches has a significant shift, it means that the center has shifted due to the long absence of a tooth after its removal, say, the 4th unit on the left.
In this case, the correction tactics are based on creating space in the side to which it is planned to shift the center. To do this, the doctor performs an extraction of the quad on the right, and a displacement is planned in this direction.
Application of elastic rods
Elastic cords are used in the treatment of dental center disorders as auxiliary elements. They cannot eliminate the problem on their own and be the basis for correction.
A correction plan based solely on orthodontic rubber bands will not bring the desired result.
Modern methods for correcting shortening of the dentition and the expected result.
This publication contains all the most important information about tooth intussusception.
Here https://orto-info.ru/zubocheliustnye-anomalii/ryadov/chto-skeletnaya-opora.html find out what absolute skeletal support is.
Surgical intervention
Surgical intervention to eliminate displacement (doctors call the rotation method) is one of the best options for effective treatment of pronounced deviations from the norm. The essence of the technique is to shift the upper jaw relative to the skull.
Features of this type:
- Making an incision in bone tissue.
- Changing the position of the upper jaw under mechanical pressure.
This type of surgical intervention helps to radically change the situation with the position of the teeth and restore the ideal center.
Prosthetics and restoration
Often, among conservative methods of treating midline displacement, experts consider aesthetic correction to be the optimal choice: prosthetics with crowns, restoration with veneers, or grinding of cutting areas followed by restoration of the integrity of the tooth with a composite.
The restoration of central incisors with wide diastemas using the method of building up the walls of the teeth is widely used. For these purposes, a polymer that is optimal for the shade of teeth is selected.
The main task of the dentist in the process of this manipulation is to bring the shape of each problem unit as close as possible to the natural one.
Classification and reasons for formation
The center of the teeth on one or two jaws at the same time may shift for the following reasons:
- disruption of the process of replacing temporary teeth with permanent ones;
- late eruption;
- TMJ diseases;
- dystopic fangs;
- lack of space in the jaw arch;
- disturbances in the development of one or both jaws;
- abnormalities in tooth size;
- traumatic injuries;
- heredity.
Let's consider an example of a clinical picture with a slight displacement.
A client of a dental clinic has a violation of the replacement of the primary canine with a permanent element on the left in the upper dentition. For this reason, the center line shifted to an empty space - to the left.
On the mobile jaw, on the contrary, there was a delay in changing the canine on the right side. Accordingly, the interincisal straight line is shifted to the place of the missing tooth to the right.
If there is a slight deficiency in the dentition, its expansion in the area of the unerupted unit will lead to lengthening of the jaw arch and a slight shift of the center in the opposite direction. But in orthodontic practice, more complex displacements of the “center of the teeth” are encountered. The optimal methods of their treatment will be discussed below.
Experts classify the anomaly into two types:
- True offset .
Orthodontists also call this type deviation or corpus displacement. The problem is characterized by a discrepancy between the upper point of the interdental papilla and the contact point of the central incisors with the approximate vertical line. This clinical picture mostly occurs due to the absence of a complete row element in the masticatory or frontal zone. In the absence of one of the frontal units, the displacement takes on a pronounced character. - False displacement is a violation of incisal angulation.
It occurs against the background of dysfunction of the mesial-distal inclination of the longitudinal axes of the anterior teeth located in the middle of the upper row. The peculiarity of the anomaly is that the vertical straight line passing through the center of the border region of the middle part of the lip coincides with the gingival papilla, while the interdental contact points are deviated from them.
Diagnostic measures
To identify the type of displacement, a photograph of a smile is assessed and the patient is prescribed an orthopantomogram. From the photo you can determine the presence of displacement and the degree of its severity. Using the second diagnostic method, the type of anomaly is determined.
If the clinic is not examined using OPTG, the problem will remain unrecognized and the patient will remain without treatment for the incorrect axial inclination of the frontal elements of the row.
The issue of correct diagnosis arises especially acutely in adult patients with increased abrasion of the cutting line of the upper jaw incisors and in children with teeth with traumatic chips.
The keys to optimally choosing treatment tactics are:
- length of the coronal part of the frontal units;
- posterior level of the occlusal plane;
- incisal platform;
- pupil lines.
If a discrepancy is detected between the line of the pupils and the incisal platform, the specialist performs a number of assessment actions:
- The relationship between the pupil line and the posterior and anterior levels of the occlusal surface is determined. If there is an obvious discrepancy, the cause of the displacement is most likely the pathological growth of the branches of the movable jaw.
- Determining the presence of a relationship between the posterior level of the occlusal plane and the pupil line. The coincidence indicates that the anomaly developed against the background of bad habits - thumb sucking, etc.
To thoroughly study the causes of the anomaly, the orthodontist must:
- Assess the morphometric parameters of the patient’s jaw apparatus and characterize his condition.
- Visually inspect the patient's jaw arches and assess the position of the units in relation to the midline of the face.
The purpose of expanding the space for the implant
Sometimes patients are interested in whether it is possible to do without additional measures and “just install a smaller prosthesis.” The answer from a competent dentist will always be negative. An artificial crown must withstand full load, and for this it must have normal dimensions and take up the same amount of space as the extracted tooth.
Thus, the doctor decides to expand the place for the implants in order to:
- eliminate possible obstacles to the installation of an artificial root and its subsequent integration with bone tissue;
- get enough space for an artificial crown, which is fixed on the implant after its implantation;
- ensure high aesthetics of the restored dentition.
Sometimes, when teeth are significantly misaligned, it may seem better to move the rest of the row to spread them out evenly and close the gap. But with this approach, the chewing load falls on fewer teeth, which means new problems will soon appear.