Technologies that make it possible to correct defects in the development of the jaw row and bite provide high effectiveness when organizing competent treatment. One popular mechanism is orthodontic plates, which allow you to focus pressure on individual teeth. Under the influence of load they shift and take the correct position. The Katz bite block is an effective way to restore the dentition and normalize the bite.
Description and characteristics
The model in question is a plastic product attached to the palate of the mouth. The work is based on the principle of pressure that occurs during the work of the masticatory muscles. The functionality that the bite block implements occurs only when the jaws close. The intensity of muscle work determines better the final result. Muscular traction that occurs due to unusual forced positioning of the jaw also affects the movement of dental units.
The bite block is attached to the upper jaw using clasps. The part of the device in contact with the frontal incisors is formed in an inclined form, at an angle of 45°, ensuring constant sliding of the teeth, due to which gradual advancement and adaptation occurs. At the same time, it does not adhere to the front part of the palate, so the teeth themselves become the main point of support.
Kappa Schwartz and Bynin
The Schwartz and Bynin mouthguards are removable functional guiding devices, since they act during movement of the lower jaw. They are located on the lower jaw, only the Schwartz apparatus covers the entire dental arch with a cast plate, and the Bynin apparatus covers only the frontal region. These devices differ from the Katz plate in that they use a vestibular arch rather than hooking loops for fixation.
The disadvantage of using these systems may be a complication in the form of disocclusion. To avoid complications during treatment with these types of devices, the orthodontist checks for the presence of the following factors:
- is there any free space in the dentition where the incisor can move;
- the initial displacement of the cutter is not very large.
Indications
The Schwartz and Bynin systems are aimed at the vestibular movement of the upper incisors and canines, in parallel with this, the distal movement of the mandibular bone is achieved. Treatment of mesial occlusion is possible when complicated by retrusion of the upper frontal teeth. Thanks to these devices, it is possible to restrain excessive development of the mandibular bone, if there is such a predisposition.
The Schwartz and Bynin designs are most often prescribed in adolescence, during the period of a replaceable or permanent set. If there are baby teeth, the method is not used.
Operating principle
The source of force when using these systems is the contractility of the masticatory muscles. Due to this, the upper incisors move and the lower jaw shifts, and the transformation can also involve the structure of the temporomandibular joint.
Design
The design has a base made of nickel silver, plastic or duralumin. This plane departs from the cutting edges at an angle of 40-65°. There are retaining clasps and a U-shaped vestibular arch.
Manufacturing
Before the manufacture of the Schwartz and Bynin apparatuses, impressions are made of the upper and lower jaws, and the impressions are placed in an occluder. Mouthguards are made in a technical laboratory. This is done using casting or stamping, depending on the material. Plastic is more inert, while in rare cases there is an allergy to metal. After manufacturing, the device is ground and polished.
On the outer walls, holes are made in the crown of each tooth. This is necessary so that the plate can be easily removed after the course is over. The system is then transferred to the dental office, where it is fixed using phosphate cement.
Activation of the Schwartz and Bynin aligners is carried out once every week and a half by correcting the inclined plane.
Purpose
At the preliminary stage, the patient undergoes a mandatory diagnostic examination, the results of which allow us to draw a conclusion about the feasibility of using the design. The priority is to correct the palatal position of abnormally growing units. The optimal age for the procedure is the period of 6-11 years, characterized by the formation of the final bite and the replacement of temporary elements of the dentition with permanent ones. If the technical conditions are met, the system allows you to align the entire jaw - for this it is necessary to maintain it in a certain position, which contributes to the development of sufficient muscle tension.
When treating adolescents, the adjustment plate gives the desired result already at the initial stage. Removable soft plastic systems are excellent for slowing or increasing the growth of individual units, adjusting the shape and position of the lower and upper jaw, and narrowing or widening the palate. The technique is successfully used to prevent prognathia, acting in two directions at once: sagittal (mesial displacement) and vertical (shortening the anterior and lengthening the lateral elements).
Lightweight and convenient plates made of plastic can be equipped with a screw, allowing you to freely change the size of the device. It is worth noting that in the first days of wearing the system will cause inconvenience to the child, interfering with speech and causing discomfort from the presence of a foreign body in the mouth. Adaptation lasts several days, after which the patient gets used to the product and stops paying attention to it.
Katz bite block
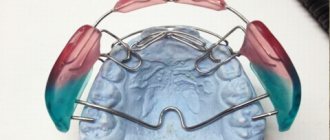
This is a removable plate for the upper jaw with flip-over clasps for its incisors. The device is strengthened using reversible clasps on the second premolars or first molars. In the anterior part of the palate, the plate does not adhere to the mucous membrane and necks of the teeth.
The Katz bite block is used in the treatment of prognathic dentition with deep incisal overlap. The effect of this device, like all bite plates with an inclined plane, is that the lower front teeth, in contact with the inclined plane, are deflected towards the lip and are partially immersed in the alveolus.
It should be borne in mind that this involves a restructuring of the bone tissue of the alveolar process, and not just the introduction or movement of teeth. In the area of the lateral teeth, which are separated, dentoalveolar elongation occurs, i.e.
Katz bite block
protrusion of teeth from the alveoli and construction of bone tissue in the vertical direction. With such a restructuring, i.e., the introduction of anterior and dentoalveolar advancement of the lateral teeth, the depth of the incisal overlap decreases. At the same time, the lower jaw moves forward and is held in this position by an inclined plane.
Prolonged protraction of the lower jaw leads to adaptive restructuring of the temporomandibular joint, jaw bones and musculo-ligamentous apparatus. As a result of this, the relationships of the jaws and dentition in the anteroposterior direction are normalized. Thus, when using plates with a guide inclined plane, a restructuring of the entire dental system occurs, leading to the elimination of the prognathic relationship of the dentition and deep bite.
The group of removable functional-guiding devices includes a plate for the upper jaw with an inclined plane and a vestibular wire arch, which is used in the treatment of prognathic relationship of the dentition with deep incisal overlap, as well as a plastic mouth guard with an inclined plane by B. N. Bynin, which is used in the treatment progeny in children.
Kappa Bynina
It covers all the teeth of the lower jaw, reaching the necks. In the area of the incisors and canines there is an inclined plane. When the dentitions close, the front teeth of the upper jaw, in contact with the inclined plane, slide along it towards the lip and are partially immersed in the alveolus. Therefore, this device is used to treat palatal inclination of the maxillary incisors, progenic relationship of the anterior teeth and false progeny with deep reverse overlap of the incisors.
When using Bynin's mouth guard in the area of separated upper lateral teeth, dentoalveolar elongation is observed, i.e., premolars and molars, together with the alveolar process, descend downwards. As a result of this, after some time the lateral teeth come into contact with the chewing surface of the mouthguard and the action of the device stops. To continue treatment, the chewing surface of the mouthguard is ground off, and thereby the bite in the lateral areas is again separated.
The force of contraction of the masticatory muscles is again transmitted to the anterior teeth of the upper jaw, which come into contact with the inclined plane and move to the labial side. When treating forced progeny with this device, along with the movement of the upper front teeth forward, there is also a slight displacement of the entire lower jaw distally, i.e., to the normal position.
“Childhood Dentistry”, A.A. Kolesov
Combined action devices
Combined action devices contain elements of mechanical and functional devices. Their design must include an inclined plane or bite pad in combination with mechanical devices (screw, spring, rubber rod, etc.). Combined action devices include: Gulyaeva apparatus; Khurgina apparatus; Bruckle's apparatus; activators of Andresen and Goipl, etc.; functional Frenkel regulators. Gulyaeva’s apparatus is used…
Apparatus of Khurgina, Bruckle, Andresen and Goipl
Khurgina apparatus The Khurgina apparatus consists of a Katz bite plate and an expanding screw, which is located in the middle of the plate. It is used to treat prognathic dentition in combination with deep bite and narrowing of the upper dentition. Bruckle's apparatus The Bruckle's apparatus is a removable plate on the lower jaw with a vestibular wire arch. In the anterior section there is an inclined…
Activator
The activator is a removable plate device that covers the mucous membrane of the hard palate, the oral surface of all teeth of the upper and lower jaws, as well as the mucous membrane of the alveolar processes on the inside. The bed for each tooth forms an inclined plane along which it can be moved forward, backward or to the side. The teeth do not come into contact with the plate with their entire internal...
Functional Frenkel regulator
The functional Frenkel regulator consists of lateral and vestibular pellets located in the vestibule of the oral cavity in the area of the lateral and anterior teeth. They relieve the dentition from the pressure of the cheeks and lips and create conditions for normal jaw growth in the transversal and sagittal directions. In addition to these pilots, the device contains elements of mechanical devices in the form of a spring for moving teeth....
Structural changes in the dental system during orthodontic treatment
Orthodontic treatment of dentofacial deformities is based on changing the mechanical and functional load on various parts of the dentofacial system. It is achieved with the help of myogymnastic exercises or the use of orthodontic appliances. Under the influence of a changed load, tissue restructuring occurs, as a result of which it becomes possible to correct the deformity. The latter involves the movement of the teeth and lower jaw in different directions, as well as the expansion of the dental...
Advantages of the correction technique
Using a correction system has a number of advantages:
- quick and effective correction of minor defects and anomalies;
- the possibility of complete hygienic oral care;
- low cost and fast production time of the structure.
The popularity of the model is due to the fact that it is one of the few devices whose use can be prescribed at an early age. Installation of braces and mouth guards is recommended after completion of the process of bone tissue formation, that is, not earlier than 12-13 years.
Types of dental crowns for chewing teeth
When choosing a material for creating a microprosthesis, you should take into account the functional purpose of the teeth.
The molars of the posterior zone of the dentofacial apparatus are subjected to strong mechanical and chemical stress when chewing food. Eating food that differs in taste, composition and hardness can quickly damage the nozzle, which is made of aesthetic material, but vulnerable to the abrasive properties of some products. In addition, the material should not cause allergies to the soft tissues of the oral cavity. Therefore, it is better to entrust the choice of material to a specialist. I am an orthopedic dentist, Sergey Samsakov, taking into account the results of the research, I recommend the optimal material option for creating a crown in each specific case:
- Metal-ceramic crowns
- a successful combination of strength, cost and beauty have made this type of onlay the most popular for installation on a tooth. Metal-ceramic crowns are installed with mandatory circular grinding of the tooth being restored.
- Metal crowns
are reliable products with a budget price. These are long-term onlays with good biological compatibility and do not require preparation of healthy tooth tissue. They can be made in combination with precious alloys. The only negative is the possibility of developing an allergic reaction. - Ceramic prostheses made of zirconium dioxide
are an ideal option for placing crowns in patients with contraindications to the use of metal structures. The high cost of the ZrO2 crown is fully compensated by the durability and aesthetics of the dentition. - Metal-plastic
dental prostheses are very fragile and are used by the doctor as temporary crowns on a tooth with the subsequent installation of a permanent crown made of durable material.
The structural reliability of the prosthesis allows you to protect the living tooth from further abrasive processes and maintain the ability to fulfill its purpose - thoroughly chewing food.
The principle of installing a crown on a chewing tooth
This is a step-by-step process, where each step takes a different amount of time and procedures preceding the placement of the prosthesis.
- Initial consultation with a dentist – examination, diagnosis of problem areas of the oral cavity. Drawing up a prosthetic plan and choosing material for making crowns;
- Preparatory measures consist of absolute sanitation of the dental system. If required, the pulp is removed and a support pin is prepared.
- Preparation of the tooth, production and transfer of a plaster model of the tooth to the denture laboratory, where a crown for the tooth or implant is created.
- Installation of a temporary metal-plastic structure.
- Fitting and temporary fastening of an element to be worn by the patient for a certain period. After the trial period (one month), if the patient has no complaints, the doctor removes the prosthesis and cleans it thoroughly. Then he places it on the support again, having previously treated it with a special medical composition.
The method of installing crowns is the same for both upper and lower chewing teeth.
What is the cost of a dental crown?
The cost of restoring a lost or defective tooth depends on many factors, the main ones:
1. The status of the dental clinic in general and the treating orthopedist in particular - the higher the doctor’s rating, the more expensive the cost and quality of the services provided.
2. Material for making a crown: the lowest price of metal products, ceramic crowns and products made of zirconium dioxide cost from 27,000 thousand rubles per unit. A crown containing precious metal is the most expensive.
All stages of preparation and treatment: consultation, hardware diagnostics, filling and other procedures that ensure oral health also require certain financial costs. The services of a dental technician are included in the final cost of installing a crown on a tooth.