Function of buttresses
Buttresses are thickened areas of bone tissue on the facial parts.
They perform the following important functions:
- Load balancing during chewing movements. In this case, not only the teeth and alveolar parts of both jaws take on the pressure, but part of it is redistributed to the zygomatic region. This reduces the impact on the teeth. They are less susceptible to destruction and last longer.
- Reducing the intensity of jolts and shaking that occurs when a person walks. Due to the upright posture that has developed in the process of evolutionary development, the head and brain, in particular, constantly experience shocks when walking and running. Some of them are cushioned by the spinal column and the peculiarities of the membranes of the brain. Some are hidden precisely by the structure of the skull, that is, by the presence of buttresses.
- It is also necessary to soften shocks when a person plays sports.
Important: In case of accidents, skull buttresses help reduce concussive forces that are destructive to the human brain.
Photos and videos in this article will demonstrate the operation of buttresses and the distribution of force load across the bones of the skull.
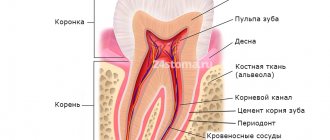
Buttresses and structural features of the skull
Bone thickenings or buttresses of the jaws alternate with thinner bony sections. These weak points are very vulnerable to physical impacts, shocks, and pressure. Most often, these places become holes in the bones, which serve for the passage of nerve fibers and blood vessels.
Upper jaw buttresses
Buttresses of the upper jaw, features of their location
The maxillary thickenings consist of four formations.
Table No. 1. Maxillary buttresses and their functions:
| Name of thickening | Location | Functions |
| Frontonasal thickening | It starts from the alveolus in which the fang is located, rises higher along the frontal process of the upper jaw, and reaches the nasal zone of the frontal bone. These right and left thickenings have additional reinforcement due to bone ridges. They are located transversely and are superciliary arches. | The purpose of these buttresses is to reduce the pressure that is generated during the operation of the fangs. |
| Alveolar-zygomatic thickening | Originates from the alveolar eminences of the first and second painters. Moves upward and to the side with the help of the zygomaticalveolar ridge. It reaches the cheekbone bone, where the excess load is redistributed. With the bone it is directed back to the zygomatic process of the temporal bone. Up, onto the zygomatic process, which belongs to the frontal bone. Inwardly, towards the zygomatic process and the infraorbital zone of the upper jaw, approaching the frontonasal buttress. Externally, this buttress is the most pronounced on the relief of the human skull. | The task is to distribute the load that occurs during the operation of chewing teeth, which is directed upward, backward and inside the jaw. |
| Pterygopalatine thickening | It extends upward from the alveolar tuberosity and maxillary tuberosity. There it is strengthened by the pterygoid process belonging to the sphenoid bone, as well as by the plate of the palatine bone. | The task of this buttress is to redistribute the force arising from the painters upward and forward. |
| Palatal thickening | Formed using the maxillary palatine processes. And the plates of the palatine bone, which connect the alveolar arches on both sides, located horizontally. | The function of this buttress is to alleviate the pressure generated in the transverse plane that occurs during chewing of food. |
Important: all buttresses are formed as a person grows; in newborns they are less pronounced than in adults.
Mandibular buttresses
Location of thickenings on the lower jaw
There are two main buttresses:
- Alveolar thickening. It starts from the lower border of the alveoli and moves upward to the gingival margin.
- Ascending thickening. It runs along the entire body of the lower jaw, reaching the condylar process. Thus, providing basic support to the entire lower jaw.
The buttresses of the lower jaw are located along the following paths, according to the course of tension arising during chewing food and movements:
- in directions from the coronoid and condylar processes to the alveolar zone;
- between the apices of the processes in an arcuate manner along the notch;
- between the mental tubercles on the right and left;
- in the interval from the mandibular angle to the peak of the coronoid process;
- fan-shaped lines of thickening follow from the retromolar recess.
We can say that the formation of thickenings is a response of the bone structure to the occurrence of overload of bone tissue.
Important: there are buttresses not only on the outer surface of the skull, but also on the inner, this provides protection from fractures and cracks under force.
Summary
Reconstruction and rehabilitation of patients with defects of the upper jaw are the most difficult in reconstructive maxillofacial surgery, occupying the minds of oncological surgeons working in this area, microsurgeons, plastic surgeons and orthopedic dentists involved in maxillofacial and somatotropic prosthetics.
The fundamental difference between patients who have undergone anatomical reconstruction of the alveolar process of the upper jaw, as well as nasal support with microsurgical grafts and patients who have undergone maxillofacial prosthetics with obturation structures is an increase in the volume of the respiratory space, improved speech, the absence of atresia, frequent acute respiratory viral infections and, fundamentally, in the absence of regular relocation of definitive orthopedic work [1]. An important difference is also the lack of mobility of dentures on dental implants, which avoids chronic trauma to surrounding tissues.
This article describes the experience of rehabilitation of patients with defects of the upper jaw using fibular and Chinese skin-bone flaps with further plastic surgery of bone and soft tissues in order to create conditions for dental implantation, orthopedic conditions and features of fixed prosthetics for this group of patients.
The developed protocols for the use of a particular graft on a vascular pedicle are described in terms of the type of defect and further restoration of bone joints, as well as measures for the formation of anatomically close to normal conditions for implantation and prosthetic dentistry in patients with a reconstructed upper jaw.
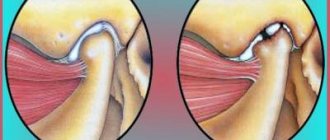
Contracture of the lower jaw
Important: all contractures must be differentiated from trismus, strong clenching of the jaws during an epileptic seizure, so the diagnosis must be made by a doctor.
Contracture is a phenomenon when a person can only close his jaw with pathological features. They are explained by changes in the elasticity of the soft tissues of the jaw, disruption of the functioning of the temporomandibular joint ligaments. Disorders occur due to a traumatic factor or disease.
Contractures are accompanied by painful sensations for the patient when working the jaws. You should consult a doctor as soon as a person feels the first sensations of pain and restrictions in the functioning of the jaws.
Self-medication for this disease is not effective, but also dangerous. After all, it is better to devote the time spent to qualified treatment; in such conditions, the cost of delay is too high.
Types of contractures
Contractures of the lower jaw occur in various situations; their type depends on the source:
- Unstable contracture is formed due to weakening of the muscles involved in chewing actions. This occurs after wearing special splints that are used to treat fractures. The reason is long-term inactivity of the muscular system of the joint. Also, unstable changes occur due to inflammation in the tissues around the lower jaw.
- Persistent contracture is formed due to the formation of scars and similar changes in the maxillofacial area, due to: a gunshot wound, a traffic accident, a fracture of the coronoid process, the zygomatic arch, due to a burn or inflammation of the tissues near the jaw. The cause of scar formation can be an oral disease - stomatitis. Diseases of the muscles involved in chewing - myositis - can also cause contracture. The neurological factor influences the formation of contracture, so hysterical states and paralysis contribute to excessively strong contraction of the jaws with subsequent injury to the perimaxillary tissues.
So, depending on the source of scar formation, the type of contracture depends:
- dermatogenic – if the scar is on the surface of the skin;
- mucosogenic – when scar tissue is concentrated in the mucous membrane;
- myogenic – if the cause is a scar in the muscle.
With complex injuries and damage, a mixture of several types of contractures is possible.
Important: contracture can occur as a complication after certain types of anesthesia during treatment and tooth extraction.
Signs of contracture of the lower jaw
If a person suffers from this disease, the following symptoms will be observed:
- a person’s speech is disrupted and distorted;
- difficulty eating;
- the line of the dentition is transformed, taking on the shape of a fan;
- an open bite is formed;
- when opening the mouth, the jaw moves towards the source of the disease, the patient is not able to move the jaw towards the absence of damage;
- If a child suffers from contracture and the formation of the jaw bones has not yet completed, the lower jaw may lag behind the upper jaw in development.
The nuances of implantation in the upper jaw
The requirements for the front teeth located in the smile zone are quite high. New teeth should look natural and beautiful, not stand out from others. When planning an operation, the dentist pays attention to the following parameters: 1. Gingival contour. Patients turn to the dentist much faster if one of the front teeth has been lost, since the resulting gap not only causes discomfort, but also disturbs the appearance. Therefore, the condition of the gums allows you to create a beautiful and smooth gum contour without additional procedures. When implanting upper front teeth, dentists often resort to one-stage implantation with simultaneous installation of a crown. A temporary crown allows you to correctly form the gingival contour and prepare the gums for the installation of a permanent prosthesis. If additional procedures are required for implantation, and the operation itself takes place in two stages, then patients are recommended to make an individual abutment and gum former for the front teeth. The gum former is installed in the upper part of the implant for 2 weeks, after which it is replaced with an abutment with a crown. If you use standard components, a gap may form between the gum and the crown. Food particles will accumulate in it, causing an unpleasant odor and inflammation. The gums on the front teeth may sag, exposing the head of the implant. Any visual defects reveal an artificial tooth; the result does not satisfy the patient, and over time can lead to plaque formation and inflammation. Therefore, the issue of aesthetics is also additional protection of the tooth from peri-implantitis.
2. Type of crown. When drawing up a treatment plan, dentists recommend using zirconium or all-ceramic crowns in the area of the front teeth. These materials are highly durable and at the same time, they visually replicate the transparency of enamel and natural shine. Only high-quality materials can convey the transparency of a tooth, so the orthopedic part of implantation of the front teeth will cost slightly more than on the lateral and chewing teeth. To make a ceramic or zirconium crown look natural, it is placed on a ceramic or zirconium abutment. The metal abutment gives a dark gray tint to the tooth and looks unaesthetic.
3. Implant installation. The alveolar ridge must have a certain thickness in order for a sufficiently strong support to surround the implant. Implantation must be as precise as possible. Whenever the implant deviates from the intended trajectory, the bone tissue wall loses strength. If there is excessive load, an incorrectly installed implant can injure surrounding tissues, become loose or fall out. To avoid inaccuracy and medical error, a surgical template is used, which maintains the desired position and prevents deviation into the area of softer tissues. Computed tomography helps to study the bone structure in detail and guide the implant in the right direction, bypassing the anatomical structures of the jaw.
4. Type of implant. For implantation into the bone tissue of the upper jaw in the frontal region, implant models with a special thread design are used. A minimally invasive effect on surrounding tissue preserves the biomaterial. Implants are smaller in length and diameter, which allows you to accurately replace your own tooth root with an artificial one.
Treatment
Foci of inflammation can be stopped with local injections
Treatment of contractures is based on treating the underlying cause of the disease.
Table No. 2. Causes of jaw reduction disorders and treatment methods:
| Reason for violation | Treatment method |
| Neurological disorders | Treatment and relief of symptoms of epilepsy, treatment of spastic paralysis and hysterical conditions. |
| Inflammatory conditions | Elimination of the source of inflammation - tooth extraction, opening of phlegmon or abscess. For inflammatory contractures, local injection of anti-inflammatory drugs into the perimaxillary tissue is used. The final part is antibiotic therapy. |
| Bone changes | Surgical treatment, resection of adhesions and adhesions are performed. |
| Scar formations | Excision of scars and insertion of triangular flaps. |
Carrying out the operation
For a person who has contracture of the lower jaw, surgical treatment is the main way to get rid of the disease if it arose due to scar formation. It is also necessary to carry out postoperative measures - mechanotherapy, therapeutic exercises, physiotherapy.
The essence of the intervention is dissection of scar formations. In this case, it is often necessary to close the wound surface. For this purpose, flaps from surrounding tissues or from the submandibular area and neck are used.
If the defect is significant and a too large piece of tissue is required, then a Filatov stem is used for replacement. If, after an injury, superficial scars have formed on the cheeks and corners of the mouth, they are eliminated using longitudinal dissection and joining the edges of the tissue prepared on the sides of the defective area.
In rare cases, when contracture occurs due to bone degenerative processes, operations are performed on the affected bone formations.
Physiotherapy
Physiotherapy is an important part of recovery
In simple cases, physiotherapy and gymnastics can be used as the main treatment method.
As physiotherapeutic support after the implementation of the main method of treatment, the following is used:
- paraffin therapy - using heated paraffin to apply to the site of the disease;
- Ultrasound therapy – application of an ultrasound source to the diseased area;
- the use of lidase and hyaluronidase, they can be used as a means for subcutaneous administration, for electrophoresis, for applications.