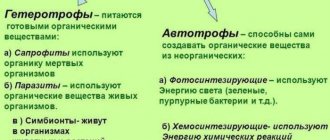
Optimal parameters
When talking about teeth of reduced size, we should mean their clinical crown, the part that protrudes above the gum.
The difficulty in classifying a particular tooth as “short” (or “small-sized”, so to speak) is that there is no value for the length or width of the crown that can be considered absolutely normal. Everything is relative.
The size of the clinical crown depends on the anatomical features of the jaws of a particular person, his age, face type and even, as it turned out, nationality. Therefore, a crown of a certain size may be “short” for one person, but normal for another.
We'll talk more about all this below. Now let’s talk about what visual signs a person can use to make a conclusion whether he has “short” crowns or not.
One of the characteristic manifestations of “short” teeth is the exposure of the gums by more than 2 mm when smiling. However, this can happen not only due to “short” crowns, but also for other reasons.
By the way, a smile with more than 3 mm of gum exposed is called “gummy”. This is considered a pathology that it is desirable to get rid of.
The patient can also determine the presence of “short” teeth by the following signs:
- Clinical crowns visually appear shorter than they should be and protrude above the gum by a small amount.
- The face looks asymmetrical. Most often this is expressed in a reduced lower third of the face.
- Wrinkles form around the mouth.
- The upper lip looks thinner when smiling compared to the lower lip.
Often reduced sizes are accompanied by the presence of trema and diastemas. Which is quite understandable, in normal-sized dental arches there is an excess of space for teeth of small width.
What is macrodentia and why is the anomaly dangerous?
Come here to learn more about microdentia in primary teeth.
At this address https://orto-info.ru/zubocheliustnye-anomalii/zubov/strukturyi-tverdyih-tkaney/displazija-emali.html all the most important things about enamel dysplasia.
Treatment and prevention of dental anomalies
It should be remembered that dental anomalies are a serious disease for patients of all ages and professions and require long-term and thorough therapy to maximize or completely eliminate dental pathologies. Modern dentistry and advanced equipment are capable (if not completely, then maximally) of eliminating the manifestations of dental anomalies. A timely visit to a specialist in order to establish an accurate diagnosis and determine a treatment plan can guarantee a favorable prognosis for recovery. Dentists will be able not only to restore the functional abilities of the jaw, but also to eliminate various aesthetic defects.
Prevention of the formation of dental anomalies begins with taking care of the correct intrauterine and postnatal development of the child. This includes:
- balanced diet;
- timely correction of endocrine disorders;
- regular visits to the dentist to carry out the necessary preventive and therapeutic measures;
It is important to monitor your own health in the first days after the birth of your child.
Early breastfeeding and a balanced diet will help avoid many dental anomalies. We should not forget about a complete preventive examination by the dentist - at least once every six months. Moscow metro station Zvezdnaya, Danube Avenue, 23
Formulas for calculating proportions
The normality of the crown part of the teeth is determined not by their size, but by the width and length of the dental arches, which are considered normal for a specific group of patients.
If the length and width of the arch correspond to the norm, and all the teeth on it are located without crowding or gaps, then their sizes are considered normal.
Many different techniques have been proposed to determine the normality of the jaw arches, taking into account the age, facial type and nationality of the patient. Three of them are discussed below - the Gerlach, Pon-Linder-Hart and Corkhouse methods.
Gerlach method
According to the Gerlach method, the dentition is divided into 3 segments:
- anterior, consisting of 4 incisors;
- two lateral ones, consisting of canines, premolars and the first molar.
Next, the calculation is made according to the following algorithm:
- The length of each segment is measured. In this case, the value of the length of the lower frontal segment is obtained by multiplying the length of the upper frontal segment by the Tone coefficient (1, 35).
- Compare the obtained lengths of the segments with each other and the tabular data compiled by Gerlach. With normal jaw sizes, they must be in certain proportions to each other.
If it turns out that the dimensions of the arches are normal, and there is no crowding or gaps, then the dimensions of the clinical crowns are normal.
Reference. All methods used involve measurements of dental arches at strictly defined points and according to certain methods. Because of their relative complexity and length, they are not included here. But they can be easily found in numerous sources.
Pon-Linder-Hart method
This technique is intended to determine the normal width of the dental arches in children with variable and permanent dentition. In this case, the formula developed by Pont is used and has the following form:
A ∶ 80 × 100 = distance between first premolars
A ∶ 64 × 100 = distance between first molars, where:
- A – total width of 4 incisors;
- 80 and 64 – Pon coefficients (indices).
Linder and Hart found that these coefficients for children of German nationality should be 85 and 65, respectively.
The algorithm for determining the parameters of the upper jaw according to Pon-Linder-Hart is as follows:
- The total width of all incisors along their cutting edge is measured.
- The obtained data is substituted into the Pon formula, and the distance between the first painters and premolars is calculated.
- The actual width of the dental arch between premolars and molars is measured.
- The measured value is compared with the results determined using the Pon formula.
- A conclusion is made about the compliance of the width of the arches and the size of the crowns with the norm.
Based on the data obtained, a treatment plan is developed. In particular, when the row in the area of premolars and molars is narrowed by more than 6 mm, it is recommended to remove some units or widen the jaw.
Corkhouse method
The Corkhouse method is based on the relationship that exists between the total width of the maxillary incisors and the length of the anterior segment of the jaw arch, measured according to a certain scheme.
The following algorithm of the Corkhouse technique is used:
- The total width of the 4 maxillary incisors is measured.
- The length of the anterior segment of the jaw arch is measured. This is done using a technique developed by Corkhouse by connecting certain points on the occlusal surface.
- The actual size of the arc segment is compared with the desired one.
Based on the data obtained, a conclusion is made that the size of the teeth and arches corresponds to the norm, and a treatment plan is developed.
Diagnostics
An experienced dentist diagnoses dental abnormalities after an external examination and questioning of the patient. To clarify the diagnosis and identify the causes of the disease, a more detailed examination of the dental system is carried out:
- The construction of diagnostic plaster models and odontometric measurements make it possible to accurately identify changes in the size of dental units and their characteristics, which indicate the presence of pathologies.
- The color and transparency of the enamel are determined using a photographic method.
- Computed tomography or teleradiography makes it possible to obtain information about the condition of abnormal dental units in order to determine further treatment tactics.
- Panoramic radiography of the jaws is an important diagnostic method
- Electromyography of the jaws helps to assess the functional state of the facial muscular system.
To carry out differential diagnosis, the patient is referred for consultation to specialized specialists: endocrinologist, otolaryngologist, geneticist. Based on the diagnostic results, the attending physician determines treatment tactics. Depending on the type of disorder and the complexity of the disease, the patient may need the help of a dentist, surgeon, orthopedist, or implantologist.
Causes of the anomaly
The reasons for “short” teeth can be many factors, both actually reducing the size of clinical crowns and creating a visual effect of their reduction:
- Heredity. “Short” teeth of parents are often genetically passed on to their children.
- Increased abrasion of occlusal surfaces , as a result of which clinical crowns become shorter. The reasons for increased abrasion can be different; this is a large independent topic.
- Inflammatory processes in the periodontium , directly or indirectly affecting the size of the clinical crown.
- Metabolic disorders in periodontal and dental tissues , including those caused by malnutrition of hard and soft tissues.
- Excessive thinness of the upper lip , in which the gums are exposed more than they should when smiling.
- Increased size of the lip frenulum , which “creeps” onto the crown.
- Gingival hyperplasia , leading to the closure of part of the crown.
- Underdevelopment of the alveolar process , leading to a lack of sufficient support for normal tooth growth.
- Radiation exposure.
- Early removal of milk jugs.
However, the most significant and common causes are still considered to be disturbances in the formation of teeth in the embryonic and childhood periods - both genetic and reactive (acquired) in nature.
For example, severe infections suffered in infancy or serious illnesses of the mother during pregnancy.
Anomalies of hard tissue structure
An altered shape, abnormal size or color of enamel is formed against the background of an abnormality in the structure of the hard tissues of the dental unit. Among such anomalies are:
- Hypoplasia (underdevelopment of tissue). The initial degree of the disorder is manifested by the presence of chalky spots on the enamel and areas where tissue deficiency is observed. Subsequently, all kinds of pits, grooves, and recesses appear on the surface of the enamel. The defect affects all teeth in the dentition.
- Hyperplasia (excessive tissue formation). Pathology also affects all teeth at the same time. It is characterized by areas where tissue growth is observed - tubercles, sagging enamel. The consequence of the pathology is a change in the shape and size of the teeth, a violation of the occlusion (the line of contact of the upper and lower jaws).
- Anomalies of amelogenesis (enamel formation) are expressed in the presence of brown or yellow spots on the surface of the teeth. Areas where the natural composition of the enamel is disrupted become especially sensitive. Microdentia develops against the background of pathology. The cause of the development of pathology is a deficiency of microelements that take part in the formation of dental tissue. Treatment consists of replenishing this deficiency. Additionally, local remineralizing therapy and physiotherapy are performed.
- Disturbance of dentinogenesis consists of dysfunction of the mechanism of dentin formation. The main symptoms of the disease are as follows: teeth become yellow-brown or grayish in color. The fragile dentin in these areas quickly wears off, causing tooth decay and then tooth loss. The disease occurs in genetically predisposed patients. The problem can only be solved by replacing the units destroyed by the disease with prosthetics.
Possible consequences
The main problem of microdentia with preserved functionality of the dentofacial apparatus is the psychological discomfort that the patient experiences when realizing his defect. This is not as harmless as it might seem at first glance.
A person’s psychological state can have a decisive impact on his quality of life, cause central nervous system disorders and even lead to physical illness.
If microdentia is accompanied by functional and organic disorders, somatic diseases are added to psychological problems. This may be a gastrointestinal disease due to poor chewing of food, asymmetry disorder and the effect of premature aging of the face when the lower third is reduced due to a low bite, etc.
Ultimately, the consequence of “short” teeth can be a general deterioration in health caused by both physical and psychological factors.
As for the influence of microdentia on the condition of the dentofacial apparatus, it can be expressed in the following:
- Displacement of the crowns distally , that is, backwards.
- Formation of tremata and diastemas , as a result of which the teeth lose stability in the mesial-distal direction and create an increased load when chewing on the periodontal ligament. It should be noted that normally all crowns have contact with each other in the proximal areas.
- Impaired diction due to the gap between the teeth and the low height of the clinical crown.
- Development of periodontitis and periodontal disease.
Summarizing all of the above, it is necessary to conclude that severe microdentia must be corrected.
How difficult and dangerous is it to remove an impacted tooth in modern dentistry?
In this publication, we will consider the features of treatment of dental anomalies - hyperdontia.
Here https://orto-info.ru/zubocheliustnye-anomalii/zubov/kolichestva/gipodentiya.html all the most important things about hypodentia.
What do we mean by sparse teeth?
Scientific terms that describe sparse teeth or spaces between teeth are diastema and trema . The diastema is the space between the central incisors, and the trema is the space between the other teeth. These terms are practically not used by patients. Usually they go to the dentist, describing this problem using expressions such as: sparse teeth, space between teeth, dental gaps, spaces between teeth, or I want neat, straight teeth. In this article we will talk about any dental space that concerns you aesthetically.
Treatment methods
In cases where “short” teeth do not affect the functionality of the dentofacial apparatus, they are a purely aesthetic problem, and their correction is determined by the patient’s desire.
But if a functional problem is added to a cosmetic problem, the doctor must recommend mandatory treatment to the patient. Its method depends on the diagnostic results.
There are three main methods of treatment. Two of them are surgical – frenulum cutting and gum grafting. 3rd – prosthetic. Sometimes orthodontic correction is performed before microdentia treatment.
Lip frenulum trimming
If the cause of “short” teeth is a long frenulum hanging over the crowns, it is trimmed and sutured. The operation is performed under local anesthesia at any age .
Gum plastic surgery
The technology is used for microdentia of several adjacent teeth. A prerequisite for gum surgery is the healthy condition of the dental and periodontal tissues in the area of the operation.
Gumplasty or gingivectomy involves excision of the edge of the gum to expose part of the clinical crown and increase its height. As a result of the operation, the position of the gum line changes.
As an additional treatment after gum surgery, remineralization of teeth may be necessary, since the less mineralized part of the crown located under the gum may have increased sensitivity to mechanical and chemical influences. That is, the patient will suffer from hyperesthesia.
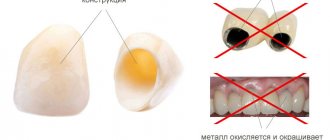
Veneers and Lumineers
Treatment of “short” teeth with veneers and lumineers is recommended for isolated, single microdentia, trema and diastema.
With the help of thin onlays fixed to the vestibular surface of the enamel, most visual defects can be corrected, and “short” teeth are no exception. Covering them with veneers and lumineers allows you to create the full effect of a normal size.
The advantage of the method is that with the help of veneering you can change the size of the crown in any direction, both in height and width. Its main disadvantage is the relatively high price, which increases when using lumineers or veneers made of high-quality materials, such as zirconium oxide, for example.
If none of the above methods are suitable for a particular case of microdentia, you can use prosthetics - installing artificial crowns or even bridges. The latter case requires the removal of a “short” tooth that cannot be corrected.
Why do gaps appear between teeth?
This image shows a case of sparse teeth that is being resolved with dental veneers. Impressions were taken using a 3Shape Trios intraoral 3D impression scanner.
Dental spaces can interfere with the proper functioning of the chewing process, especially when the cause is acquired rather than natural. Before you close the gaps between your teeth, you need to know the factors that caused them to appear:
- Congenital factor
- Incorrect occlusion (uneven contact surfaces overload certain groups of teeth and, consequently, tremors occur)
- Some forms of dental anomalies (when teeth, usually the first premolars or lateral incisors, do not erupt into the dental arch)
- Migration of teeth after extraction
- Defective skills (when the tongue pushes the teeth forward with constant pressure)
- Pathology such as periodontitis or osteoporosis (bone loss leads to changes in the dentition)