Braces are metal clasps that are attached to the teeth. But they themselves do not correct the position of the teeth - the braces system does this. The main element of the system is the arc. It is this that affects the teeth, causing them to move. To do this, the arch is changed several times during the treatment process.
Arches for braces are made of a metal alloy. Most often it is nickel and titanium or titanium and molybdenum. At the request of the patient, you can choose an arch with a white coating - it visually goes well with ceramic or sapphire braces and is almost invisible. True, the white coating wears off quickly, so such an arch can be considered more as an option for a special occasion, for example, a wedding or graduation.
With a white arch, transparent braces are almost invisible
Basic properties of the arc:
- Strength. Braces can come off from the teeth, especially if you do not follow the rules of nutrition (gnaw nuts, crackers). But it is almost impossible to break or bend the arc.
- Flexibility and resilience. Regardless of what position the arch takes, it will tend to its original shape, similar to half an oval (except for the arch of lingual braces - it repeats the shape of the regular dentition not from the outside, but from the inside, so it looks different).
No matter how bent the arch is at the beginning of treatment, it tends to return to its shape
- Hypoallergenic. The arc is made of a material that does not cause allergies and a metallic taste in the mouth. It is not magnetic and does not “ring” at the airport when going through security.
Why are the arcs different in cross-sectional shape?
All arches for vestibular brace systems differ in thickness and cross-sectional shape. And this difference is important in the process of correcting the bite.
Arcs vary in thickness and cross-section
At the beginning of treatment, an arch with a circular cross-section is installed. She is the thinnest. It is inserted into the grooves of the bracket, which are rectangular on the inside. Therefore, the round arc does not completely fill the grooves.
The fact is that by the start of treatment, the patient’s teeth have been in the wrong position for 10–20 years or even longer (depending on how much time has passed since the formation of a permanent bite). Therefore, in the first month of treatment you should not exert too much pressure on them - this will cause great discomfort. First you just need to start moving your teeth.
The thinner the arch, the less space it takes up in the bracket grooves and the softer the effect on the teeth.
After 1–2 months of wearing braces, the roots of the teeth are already in a more mobile state. Many patients feel as if their teeth are loose. This is only partly true: the teeth do move, but the loosening is limited by the braces system and is not worth worrying about.
But now you can install a more rigid arch with a square cross-section. It fills the grooves of the braces more tightly, but still not completely. Square arches are used for several months during the main stage of treatment.
Square arch braces
At the final stage, it is the turn of the rectangular arc - the thickest and toughest. It completely fills the grooves of the braces, fixing the position of the teeth. This arch is put on when the desired result is achieved. Its function is to stabilize the teeth.
Braces cannot be removed immediately after teeth are straightened. You need to go through one more stage of treatment to consolidate the result. Patients go through this stage emotionally difficult: the teeth are already straight, but the braces are not removed and the arch is thick and noticeable. But this is necessary for complete treatment.
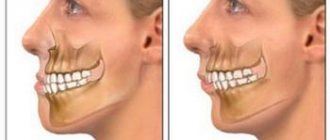
Malocclusion
The position of the dental arches relative to the central occlusion in dental practice is called occlusion. In medical practice, there are two types of occlusions – physiological and abnormal. The first type is characterized by the fact that the upper row of teeth covers the lower one. In the presence of an abnormal bite, the relationship between the upper and lower arches is disrupted. In total, there are 4 malocclusions:
- open;
- cross;
- distal;
- mesial;
- deep bite
It is important to change the arc on time
At each stage of treatment you need to get a certain result. Once it is reached and the teeth have assumed their new position, the archwire no longer works. And if you often postpone doctor's appointments, each week of delay prolongs the entire treatment.
Wearing one archwire for too long does not harm your teeth, but it does not make sense.
Treatment by an orthodontist requires self-discipline. Be prepared to adjust your schedule around your doctor's appointments. And remember that all this is done for the sake of health and a beautiful smile. And this is the best incentive!
Reasons for changing the arc
Dental defects can be the result of many unfavorable factors. The formation of arches is influenced primarily by heredity. Also, anomalies can result from various formation disorders during embryonic development. Other reasons due to which the upper and lower dentition may be deformed:
- trauma to the maxillofacial area (impact, fall);
- inferiority of the temporomandibular joint;
- presence of bad habits in childhood;
- the presence of some systemic pathologies that affect the condition of the bone tissue in the jaw, etc.
Regardless of what caused the dental anomalies to develop, it is important not to let the disease take its course, but to contact a dental clinic for advice and the development of a treatment plan.
Treatment of anomalies in the relationship of the dental arches
Treatment is preceded by an examination and a full diagnosis: the relationship of the dentition is assessed (based on impressions taken), orthopantomogram data, CT scan, etc.
Treatment tactics depend on the diagnosis and other circumstances, including age. With timely treatment, bite pathologies can be dealt with quickly. When treating young children, sometimes it is enough to stimulate proper jaw growth.
It is worth noting that age is not a contraindication or limitation for correcting the bite, but it does impose its own characteristics: first of all, we are talking about the duration of treatment and the choice of methods and devices.
Medical Internet conferences
L.V. Muzurov – Saratov State Medical University named after. IN AND. Razumovsky Ministry of Health of Russia, Professor of the Department of Human Anatomy, Doctor of Medical Sciences, Professor; M.V. Mikheev - Saratov State Medical University named after. IN AND. Razumovsky Ministry of Health of Russia, Department of Human Anatomy, postgraduate student; V.V. Konnov – State Budgetary Educational Institution of Higher Professional Education Saratov State Medical University named after. IN AND. Razumovsky Ministry of Health of Russia, Head of the Department of Orthopedic Dentistry, Doctor of Medical Sciences, Associate Professor; S.N. Sheludko - Saratov State Medical University named after. IN AND. Razumovsky, Ministry of Health of Russia, Department of Human Anatomy, postgraduate student.
Summary
Purpose: to study the variability of the parameters of the dental arch of the lower jaw in women with different face shapes. Material and methods. The study of the morphometric parameters of diagnostic jaw models was carried out in 92 women aged 21 to 51 years. For all those examined, the shape of the face (morphological index) was determined according to Garson (1910): very wide face (hypereuryprosopic); wide face (euryprosopic); middle face (mesoprosopic); narrow face (leptoprosopic); very narrow face (hyperleptoprosopic). Results. The width of the dental arch of the lower jaw at the level of premolars and molars has the largest average values in mesoprosopic women, and the smallest in hyperleptoprosopic women. The largest average values of the length of the dental arch are characteristic of leptoprosops, and the smallest - hypereuryprosops. The length of the anterior segment of the dental arch has a maximum average value in hypereuryprosops and euryprosops, and a minimum in hyperleptoprosops. In all groups, regardless of the shape of the face, flattening of the anterior segment of the dental arch of the lower jaw is determined. The greatest degree of flattening is characteristic of hyperleptoprosops. The largest average width of the basal arch is characteristic of mesoprosops, and the smallest - hypereuryprosops. In the group of hypereuryprosopians, a narrowing of the basal arch of the lower jaw of the first degree is determined. The length of the basal arch has the largest average value in hypereuryprosops, and the smallest in mesoprosops. In all groups, regardless of the shape of the face, a shortening of the length of the basal arch of the lower jaw is determined, most pronounced in meso- and leptoprosopians. Conclusion. The data obtained must be taken into account when conducting orthodontic and orthopedic treatment, when giving lectures and conducting practical classes at the departments of human anatomy and departments of dental specialization.
Introduction. In practical dentistry, the private constitution represents the characteristics of the skull that must be taken into account when carrying out treatment. Many studies have proven the influence of structural features of the skull and face on the dental system. The features of the jaws that determine the individuality of the face are also noted.
Purpose of the study: to study the variability of the parameters of the dental arch of the lower jaw in women with different face shapes.
Objects and methods of research . The study of the morphometric parameters of diagnostic jaw models was carried out in 92 women aged 21 to 51 years, who are indigenous residents of the Saratov region. To determine cephalometric parameters and measurements of diagnostic jaw models, a standard set of anthropometric instruments that passed metric testing were used: small thick and sliding compasses (with a millimeter scale); technical electronic caliper with a division value of 0.01 mm. For all those examined, the shape of the face (morphological index) was determined according to Garson (1910) - the ratio of the morphological height of the face to the width of the face in the area of the zygomatic arches × 100. According to this index, the following types of faces were distinguished: very wide face (hypereuryprosopic) - index 78.9 and less; wide face (euryprosopic) – index 79.9-83.9; average face (mesoprosopic) – index 84.0-87.9; narrow face (leptoprosopic) – index 88.0-92.9; very narrow face (hyperleptoprosopic) – index 93.0 or more.
Results. The width of the dental arch of the lower jaw at the premolar level in women with different face shapes ranges from 32.0 mm to 43.0 mm. The highest value of the parameter is determined in women with a mesoprosopic face type (37.0 mm). In other groups the parameter is smaller: in hypereuryprosops by 0.8 mm (P>0.05); in euryprosopes by 0.9 mm (P>0.05); in Leptoprosopus by 0.6 mm (P>0.05); in hyperleptoprosops by 2.2 mm (P<0.05). The lowest value of the parameter is determined in women with hyperleptorosopic facial type (34.8 mm). In all selected groups, the parameter varies slightly (CV = 4.9-9.3%).
The width of the dental arch of the lower jaw at the level of the molars ranges from 42.0 mm to 58.0 mm. The highest average value of the parameter is determined in women with a mesoprosopic face type (52.8 mm). In other groups, this parameter is less: in hypereuryprosops by 1.4 mm (P>0.05); in euryprosopes by 2.2 mm (P<0.05); in Leptoprosopus by 3.1 mm (P<0.05); in hyperleptoprosops by 4.2 mm (P<0.05). The lowest value of the parameter is determined in women with a hyperleptoprosopic type of face (48.6 mm). In all groups the parameter varies slightly (CV=5.9-7.4%).
The length of the dental arch of the lower jaw in women with different types of faces ranges from 83.0 mm to 115.0 mm. The highest value of the parameter is determined in leptoprosopus (96.6 mm). In other groups the parameter is smaller: in hypereuryprosops by 4.6 mm (P<0.05); in euryprosopes by 1.0 mm (P>0.05); in mesoprosopians by 3.3 mm (P<0.05); in hyperleptoprosops by 2.1 mm (P<0.05). The lowest value of the parameter was found in women with hypereuryprosopic facial type (92.0 mm). In mesoprosopians the parameter varies slightly (CV=8.1%), in other groups it varies moderately (CV=11.1-12.1%). Analysis of the correspondence of the length of the dental arch of the lower jaw to the sum of the mesio-distal dimensions of 12 teeth showed that for all types of faces in women, the length of the dental arch is greater than the sum of the mesio-distal dimensions of 12 teeth. The index of the dental arch of the lower jaw in women with different types of faces ranges from 37.1 to 65.9. The highest average value is determined in hypereuryprosops (56.2), the lowest - in leptoprosops and hyperleptoprosops (51.9).
The length of the anterior segment of the dental arch of the lower jaw in women with different face shapes ranges from 6.8 mm to 13.4 mm. The highest values of the parameter are determined in the group of hypereuryprosops and euryprosops, having almost equal average values in these groups (10.6 mm and 10.7 mm, respectively). In other groups the parameter is smaller: in mesoprosops and hyperleptoprosops by 2.0 mm (P<0.05); in Leptoprosopus by 0.9 mm (P>0.05). In the group of mesoprosops and hyperleptoprosops, the parameter is the smallest and has equal average values (8.8 mm and 8.7 mm, respectively). In all groups the parameter varies averagely (CV=14.3-18.4%). In all groups, flattening of the anterior segment of the dental arch of the lower jaw is determined.
The length of the lateral segment of the dental arch of the lower jaw in women with different types of faces ranges from 21.4 mm to 43.6 mm. The study showed that in all groups there were no bilateral differences and no statistically significant differences for different facial types.
The width of the basal arch of the lower jaw in women with different types of faces ranges from 32.5 mm to 40.6 mm. The highest value of the parameter is determined in mesoprosopes (36.1 mm). In other groups the parameter is smaller: in hypereuryprosops by 2.1 mm (P<0.05); in euryprosopes by 1.6 mm (P<0.05); in Leptoprosopus by 0.5 mm (P>0.05); in hyperleptoprosops by 1.0 mm (P>0.05). The lowest value of the parameter is determined in hypereuryprosops (34.0 mm). In all groups, insignificant variability of the parameter was revealed (CV = 7.7-9.9%). In hypereuryprosopus and leptoprosopus, a narrowing of the basal arch of the lower jaw of the first degree was revealed.
The length of the basal arch of the mandible in women with different face shapes ranges from 27.3 mm to 38.8 mm. The highest and almost equal average values are determined for hypereuryprosops (31.9 mm) and hyperleptoprosops (32.0 mm). In other groups, the parameter is slightly and statistically insignificant (P>0.05) less: in leptoprosopes by 0.1 mm; in euryprosopes by 0.9 mm; in mesoprosopes by 1.0 mm. The lowest value of the parameter is determined in mesoprosopes (31.0 mm). In all groups, insignificant variability of the parameter was revealed (CV = 5.9-9.9%). In women with different types of faces, shortening of the basal arch of the mandible was revealed in all groups.
Discussion. There is no data in the literature on the variability of the morphometric parameters of the dental arch of the lower jaw in women with different face shapes. The available data characterize these parameters only in connection with the identified occlusions.
According to the literature, the width of the dental arch of the lower jaw at the premolar level averages 22.2-25.5 mm [1]; varies from 28.0 mm to 43.0 mm and averages 37.0 mm [2]. According to our data, in women with different face shapes, the parameter ranges from 32.0 mm to 43.0 mm and averages 36.1 mm. The data we obtained is greater than the data given in the literature.
According to the literature, the width of the dental arch of the lower jaw at the level of the molars varies from 42.81 mm to 53.41 mm [3, 4]; from 56.0 mm to 67.5 mm (X = 50.7 mm) [5]; from 47.62 mm to 56.26 mm (X = 51.6 mm) [6]; 29.9-34.5 mm [1]. In adults, according to the literature, the parameter is on average 37.9 [7]; 52.4-56.3 mm [8]; is in the range from 53.7 mm to 62.2 mm [9]. According to our data, in women with different face shapes, the parameter ranges from 42.0 mm to 58.0 mm and averages 50.6 mm. Our data coincide with the data of S.S. Rtishcheva (2012) [8].
According to the literature, the length of the dental arch of the lower jaw in adults varies from 106.9 mm to 113.5 mm [10], is in the range of 98.6-106.9 mm [8], and averages 95.5-100 .3 mm [3], varies from 82.0 mm to 110.0 mm and on average is 94.3 mm [7]. According to our data, in women with different face shapes, the parameter ranges from 83.0 mm to 115.0 mm and averages 94.4 mm. Our data coincide with the literature data.
According to the literature, the length of the anterior segment of the dental arch of the lower jaw in adults ranges from 8.9 mm to 10.3 mm [3]; from 5.4 mm to 16.3 mm and an average of 10.4 mm [7]. According to our data, in women with different face shapes, the parameter ranges from 6.8 mm to 13.4 mm and averages 9.7 mm.
According to the literature, the width of the basal arch on the lower jaw in adults averages 35.8-39.3 mm [3]; is in the range of 32.4-43.4 mm and on average is 36.6 mm [7]. According to our data, in women with different face shapes, the parameter ranges from 32.5 mm to 40.6 mm and averages 35.1 mm.
According to the literature, the length of the basal arch of the mandible in adults averages 30.6-33.8 mm [3]; is in the range of 25.5-39.8 mm and on average is 32.4 mm [7]. According to our data, in women with different face shapes, the parameter ranges from 27.3 mm to 38.8 mm and averages 31.6 mm.
Conclusion. The width of the dental arch of the lower jaw, measured at the level of premolars and molars, has the largest average values in mesoprosopic women, and the smallest in hyperleptoprosopic women. The largest average values of the length of the dental arch of the lower jaw are characteristic of leptoprosops, and the smallest - hypereuryprosops.
The length of the anterior segment of the dental arch of the lower jaw has a maximum average value in hypereuryprosops and euryprosops, and a minimum in hyperleptoprosops. In all selected groups, regardless of the shape of the face, flattening of the anterior segment of the dental arch of the lower jaw is determined. The greatest degree of flattening is characteristic of hyperleptoprosops.
The largest average width of the basal arch of the lower jaw is characteristic of mesoprosops, and the smallest - hypereuryprosops. In the group of hypereuryprosopians, a narrowing of the basal arch of the lower jaw of the first degree is determined.
The length of the basal arch of the lower jaw has the largest average value in hypereuryprosops, and the smallest in mesoprosops. In all groups, regardless of the shape of the face, a shortening of the length of the basal arch of the lower jaw is determined, most pronounced in meso- and leptoprosopians.
Conflict of interest. The work was carried out as part of the research work of the Department of Human Anatomy and the Department of Orthopedic Dentistry, Saratov State Medical University named after. IN AND. Razumovsky, Ministry of Health of Russia.
Application of a facebow in prosthetic dentistry
Orthopedic dentists use different tools in their daily practice, one of them is the facebow. It is used in combination with an articulator.
Using an arch, the relationship between the upper jaw and the patient's skull is determined and transferred to the articulator. The dentition of the upper jaw is oriented relative to the temporal joint of the lower jaw.
Using these orthopedic devices, the dentist accurately simulates the movements of the lower jaw.
Face bow design
It consists of several elements: a main frame in the shape of the letter U, a bite fork, stops (ear or articular, as well as nasal), a transition device between the frame and the fork, and a plane indicator.
The frame (arch) goes from the temporal joints of the lower jaws to the central upper incisors. The device moves 2–3 cm away from the skin.
of supports - ear and joint. The first come into contact with the skin in the area of the external auditory canals, the second - in the area of the temporal joints of the upper jaw.
The bite fork is attached to the dentition.
Functions of an orthopedic arch
Using the device, orthopedic dentists perform spatial modeling and:
- The occlusal planes are aligned;
- The location of the dentition at rest and in motion is conveyed with high accuracy;
- A perfectly fitted prosthesis is made.
It takes no more than 2 minutes to measure.
Types of face bows
There are two types of instruments: average anatomical and kinematic.
The mid-anatomical or portable arch is a standard device that is attached to the patient’s head using stops (nasal or temporal) at the point of the axis of rotation of the condyles. Next, a bite pad with impression material is attached to the device and placed in the patient’s mouth. The structure is fastened with screws and the device is adjusted to obtain an accurate model.
An arch of this type is used if the patient is missing all his teeth - it is used to make removable dentures.
The kinematic or axial arc is fixed on the chin and forehead. It measures how the jaws and axes relate as they move.
This type of archwire is used in the manufacture of elastic and partial dentures.
How to work with an arc: 3 ways
The device is not an alternative to other prosthetic procedures, such as taking impressions, measuring jaw relationships and measuring centric occlusion. It is used as an additional procedure in the manufacture of a prosthesis. There are 3 ways to use a facebow. Let's look at each of them.
1st method: installation at the point of rotation of the condyle
For a mid-anatomical joint transfer, follow these steps:
- Find the center of rotation of the condyle. Guide yourself along the line that connects the outer corner of the eye and the apex of the tragus of the ear, approximately 1.3 cm anterior to the external auditory canal;
- Place the joint stop at the found point.
This way you will determine the real axis of rotation of the mandibular condyle with an error of 0.2 cm.
Method 2: the easiest installation
This is the simplest method, therefore the most popular. The main feature is that the arch and articulator must have sockets for fixing the arch, both from the external auditory canal and the joint.
It is important that the distance between the nests is strictly 1.3 cm.
The easiest way to install the arch is along the external auditory canal. To do this, fix the bite fork on the dentition of the upper jaw.
The use of an average anatomical arch gives an approximate transfer of the position of the upper jaw and the axis of rotation of the lower jaw.
Using an axial arc will result in more accurate results.
3rd method: using an axial arc
It is necessary to find the central position of the articular head in the joint, which ensures the central relationship of the jaws.
Use axial arc:
- Fix it on the dentition of the lower jaw;
- Ask the patient to move the jaw back and forth and open and close;
- At the same time, notice how the tip of the joint stop moves;
- Determine the axis of rotation of the lower jaw. Record when the stop indicators begin to rotate around their axis when the mouth opens 2.5 mm. This will be the axis of rotation of the lower jaw;
- Mark it on the skin with a dot;
- Transfer the upper jaw model.
The procedure is performed in the same way as we described in method 1.
Advantages of the device
The tool eliminates erroneous orientation when forming the occlusion of the model and prosthesis. This is its main advantage.
The device allows:
- Quickly, simply and accurately identify all the nuances of the jaw relationship;
- To produce high-quality prostheses - accurate and aesthetic;
- To make prostheses taking into account all the anatomical features of the patient.
- If an orthopedic dentist works with a facebow, patients also benefit:
- Save time. There is no need to visit an orthopedist for additional measurements and adjustment of the prosthesis;
- Easy adaptation. A perfectly fitted prosthesis does not take long to get used to. The adaptation period is as comfortable as possible: without pain, discomfort, rubbing, etc.;
- Rapid restoration of chewing functions;
- Durability of dentures. The load on the dentures is distributed evenly, so they will last a very long time.
Thanks to high-quality dentures, the patient’s crowns and “natural” teeth do not wear out longer.
Consequences of not using an arc
If the dentist does not use a facebow, he risks making gross errors in the manufacture of prostheses due to incorrect orientation of the models in the articulator and determination of occlusion.
Here are the most common mistakes dentists make:
- Incorrect spatial location of the upper jaw model in the articulator. The cusps of the upper jaw should correspond to the movements of the lower jaw. This is possible with their tilt angle of 35 degrees, which can be achieved using a face bow. If the device is not used, the angle of inclination will be greater - the bumps may chip.
- Discrepancy between the patient’s real occlusal paths and those on the model. If a facebow is not used, these paths will not correspond to each other, as a result of which the cusps of the lateral molars on the denture may chip.
Thus, in modern prosthetic dentistry, to produce high-quality restorations, it is advisable to use a facebow in combination with an articulator.