Normally, a person grows 52 teeth over a lifetime: 20 milk teeth and 32 permanent teeth. Supernumerary teeth are “extra” dental units that appear in addition to some incisors, canines, premolars or molars. In various medical sources, the phenomenon is called hyperdontia, supradontia or polyodontia. A superset can include 1–2 teeth or reach several hundred dystopic structures, be true or false.
Supernumerary teeth: causes of anomaly
The main cause of polyodontia is a violation of the formation or development of tooth germs. Doctors are considering several theories for this phenomenon:
- Heredity – hyperdontia develops as a result of genetic abnormalities that can be transmitted from parents to children. In this case, the pathology should manifest itself in the patient’s closest blood relatives.
- Splitting of the root germ of the tooth in the embryonic period of development. Usually observed after the mother becomes ill during pregnancy. Characteristic of single supernumerary teeth (1–2 pcs.).
- Failure during the embryonic period of tooth formation with the formation of multiple dental buds (up to several hundred). It is observed when the mother lives in unfavorable environmental conditions, during treatment with dangerous drugs, taking drugs, or alcohol abuse.
In more rare cases, polyodontia develops as a result of odontoma, a benign tumor in the area of the jaw arches. The disease is typical for children and young people during the period of active growth of tooth germs. Such a tumor structure may contain several tens or even hundreds of highly deformed dentin-enamel formations.
Provoking factors in the prenatal period:
- malfunction of genes - primarily the Msx1 gene (responsible for the formation of tooth germs);
- viral infections;
- taking teratogenic and potentially dangerous drugs;
- smoking, drug use, alcohol use;
- poor environmental conditions;
- exposure to radiation - not only direct exposure, but also increased general background radiation in the place of residence/work.
Reference! Some scientists consider the presence of supernumerary teeth as an atavism. Thus, it has been scientifically proven that various species of the genus Homo could boast a set of teeth of 36–44 pieces. However, this theory does not explain in any way the appearance of multiple rudiments covering all spaces of the sky (a typical example is an Indian boy who had to remove 230 supernumerary units).
Types of crowns
- Plastic (metal-plastic)
– plastic crowns for chewing teeth are indicated exclusively for temporary prosthetics. They are susceptible to chipping, accumulate food pigments, provoke inflammation and allergic reactions. The maximum service life is about 2 years. - Metal
– strong, corrosion-resistant, durable. One of the main advantages is that they do not require deep preparation of dental tissues. Disadvantages - low aesthetics, abrasion of the enamel of the antagonist tooth, risk of galvanic effect, allergies (excluding products made of gold and other precious metals). The high strength of the metal alloy ensures a long service life. If you place a crown on a chewing tooth made of metal alloys, it can last for several decades. - Metal-ceramic
- a metal base with a ceramic lining, they are distinguished by good aesthetics and durability, but require serious grinding of hard fabrics. Metal-ceramic structures are quite aesthetic, inexpensive, and have a long service life - 12-15 years or more. Disadvantages - rapid abrasion and damage to the enamel of opposite teeth, cracks, chips of ceramic veneer, metal showing through at the edge of the gum (gray neck). - Metal-ceramics on a gold frame
- such restorations are an order of magnitude more expensive than conventional metal-ceramic structures, but they have many advantages - they do not cause allergies, have bactericidal properties, and do not oxidize. Gold alloys can withstand high mechanical loads, while the plasticity of the material makes it possible to create very thin, yet strong structures that fit precisely to the tooth. The warm shade of gold is close to the color of natural dental tissues. Thanks to ceramic veneering, such restorations are not inferior in aesthetics to metal-free structures (zirconium, ceramic). - Zirconium
– ultra-strong, lightweight, durable zirconium dioxide restorations allow you to achieve a natural tooth appearance. Such crowns retain their original properties throughout their service life, which is 20-25 years or more. White material with a high degree of transparency, identical to the internal tissues of the tooth, allows you to create beautiful restorations with excellent performance and aesthetic characteristics. They fit tightly to the supporting element, do not require deep grinding of dental tissues, and are absolutely inert to temperature and chemical influences. - Ceramic
- classic crowns made of solid ceramic mass (porcelain) are not placed on premolars and molars. Such restorations are almost impossible to distinguish from natural teeth, but they are significantly inferior in strength to metal or zirconium ones. Therefore, they are mainly used in prosthetics of the smile area.
A - gold, B - metal-ceramic, C - zirconium, D - metal-plastic
Ceramic crowns can be installed on chewing teeth if metal-free leucite ceramics E-max (lithium disilicate) are used for their manufacture. Their durability and appearance are identical to natural enamel. They do not cause allergies and do not deform under chewing load. The minimum thickness of the restorations avoids excessive preparation during prosthetics. They are manufactured in two ways - by pressing under high pressure and temperature conditions or using CAD\CAM technology.
Symptoms of pathology
The main symptom is the presence of teeth beyond the natural set. They can have different positions, shapes and numbers. The process of teething of abnormal teeth is often accompanied by pain, fever, and inflammation of areas of the oral cavity. If measures are not taken in a timely manner, complications may develop:
- redness and swelling at the site of the impacted tooth;
- problems with chewing food and digestion;
- injuries to the mucous tissues of the oral cavity;
- violation of the position of the main teeth (dystopia) and the formation of malocclusion;
- various speech defects - mainly problems with the pronunciation of hissing sounds;
- loosening of adjacent normal teeth;
- deformation of the jaw bones.
In young children and adults, the pathology has its own nuances. They are associated with age-related characteristics of the body and affect the subsequent development of maxillofacial structures. Statistics on the spread of pathology in children and adults:
- 60% of cases are children and adolescents during the period of replacement of milk teeth with permanent ones;
- 35% of cases are adults;
- 5% of cases are small children during the period of growth of baby teeth.
Reference! Supernumerary teeth, as a rule, have a standard structure, sometimes with a smaller crown size. Less common are deformed formations of a teardrop-shaped, lumpy, chisel-shaped form.
Second lower molar
Average age of teething: 11-13 years
Average age of root formation: 14-15 years
Average length: 19.8 mm
The crown is somewhat smaller in size than the first molar, and the more symmetrical second lower molar is characterized by a close arrangement of roots. The roots gradually converge distally and have closely spaced apices.
Exposure is made at the mesial portion of the crown with access extending only slightly distal to the central sulcus. After trephination of the cavity with a fissure bur with a cutting apex, an elongated ball-shaped bur is used to expand it until free access is achieved. The distal root angles often allow for a smaller opening than the lower first molar.
Particular attention should be paid to the shape of the mouth of the distal canal. A narrow oval orifice indicates the presence of a slit-like lumen in the distal canal, which requires more careful treatment.
All carious tissue, leaking fillings and denticles should be removed and replaced with a suitable temporary filling prior to endodontic treatment.
The lower second molar is most susceptible to vertical fractures. After preparing the access, but before starting endodontic treatment, the clinician should examine the floor of the pulp cavity using fiber optics. For mesial-distal crown or root fractures, the prognosis is extremely unfavorable.
To avoid vertical fractures after endodontic treatment, it is necessary to completely cover the cusps with a restorative structure.
Features of polyodontia in children
Possible symptoms of hyperdontia in childhood:
- intrauterine formation of teeth (a child is born with several teeth);
- the appearance of teeth in the first months, weeks and even days of life;
- delayed eruption of baby teeth.
This has unpleasant consequences:
- problems with feeding the baby - he does not latch onto the nipple well and sucks weakly;
- swelling of the mucous tissues can spread to the nasal area and cause breathing problems;
- poor closure of the dental arches causes severe salivation;
- a prolonged increase in temperature to 38C is possible.
Hyperdontia is especially harmful during the period of speech formation. Teeth located outside the general row prevent the tongue from taking the correct position when pronouncing most consonant sounds. Without eliminating the pathology, any speech therapist will be powerless.
In addition to true hyperdontia, children (less often adults) can develop the so-called false form of the disease. It is characteristic of the period of tooth change and develops during the eruption of molars next to the milk teeth that have not yet fallen out. This is a fairly common phenomenon that usually goes away on its own as the dentition finally forms. In some cases, orthodontic treatment may be required.
Features of polyodontia in adults and adolescents
In adults, after complete replacement of complete teeth, the presence of additional units can lead to additional pathologies:
- chronic rhinitis, sinusitis when the wall of the maxillary sinuses is perforated by the roots of supernumerary impacted structures;
- interdental caries - due to teeth fitting too closely to each other.
Retention and dystopia
Adults are characterized by 2 main types of supernumerary teeth:
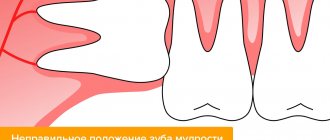
- Dystopic teeth are the name given to teeth with deviations in the direction of growth. The peculiarities of the formation of supernumerary units very often lead to dystopia. This is due to the fact that the space on the dental arch line is limited, and the roots of normal teeth simply push the “intruder” towards the cheek or palate.
- Impacted teeth – impaction occurs when a tooth loses its growth impulse and remains embedded in the jawbone. Impacted teeth can cause the adjacent normal teeth to become loose and cause them to shift and change the bite. Often cause pain.
On a note! According to statistics, hyperdontia accounts for up to 2% of cases of dental problems. Of these, 70% are associated with the appearance of single supernumerary teeth, 25% with a couple of such formations, and only in 5% complex multiple complexes of 3–4 or more teeth can be found.
Diagnostic methods
The main indication for diagnosis is the presence of an “extra” tooth in the patient’s oral cavity or obvious signs of its eruption (painful tubercle or swelling in the gum or palate). All of these signs can be identified through a routine visual examination, during which the dentist evaluates the condition of the oral cavity. To confirm the diagnosis and carry out differential diagnosis, an X-ray examination is performed - an orthopantomogram. If it is necessary to examine the dentition in several planes, computed tomography (CT) is additionally prescribed.
On a note! The patient may not be aware of the presence of impacted supernumerary teeth. In this case, hyperdontia is detected only by the results of an X-ray or CT scan of the maxillofacial region.
The recipe is ready
That's all, in short, what is needed to create teeth. Thus, the recipe for creating a tooth looks something like this:
- Stem cells - assorted
- Scaffold is a natural product
- Growth factors - to taste
Regenerative medicine technologies are progressing incredibly quickly. And now, probably, the most basic provisions for dental tissue engineering have already been developed. They all stem from our knowledge of the cellular and molecular basis of tooth development. We understand that the best result in tooth bioengineering can be achieved only in the presence of two types of cells, and not one: these are both epithelial cells and mesenchymal cells (where would we be without them?) [28]. However, you cannot build a tooth on cells alone. Thus, the role of growth factors and extracellular matrix cannot be excluded here. Fortunately, science does not stand still, and new provisions are being actively developed. Perhaps, in the near future, the treasury of knowledge called “dental tissue engineering” will be replenished with another equally valuable “coin”.
But, despite all the promising potential of tissue engineering in dentistry, there are still problems to be solved related to the conduct of clinical trials, the innervation and blood supply of the bioengineered tooth, its ligamentous apparatus, the timing of its eruption, as well as the choice of a pool of stem cells and technology for working with them , and a number of other equally pressing tasks [10], [29].
As for the most basic thing, namely stem cells: in the experiments performed (it is worth noting that almost all of them were carried out on mice), they mainly used embryonic stem cells. But in the clinic their use is sharply limited, including by law. Therefore, only postnatal stem cells remain (not counting iPSCs, where things are also not calm), and here we face the following snag: unlike mice, humans lack a niche of dental stem cells, which is why our teeth do not have the ability to constantly grow. Those MSCs that are suitable for use cannot be obtained without damaging the tooth, or even more so if the tooth was previously treated endodontically, that is, with pulp removal. Those to which access is open do not have odontogenic competence, for example, gingival MSCs. This is just one of the dilemmas that remain to be resolved (Fig. 9).
Figure 9. The fight for healthy teeth for humanity.
website accuratedentistry.net
Do supernumerary teeth need to be removed?
There is no clear answer to the question of what to do with “extra” teeth. Much depends on the shape, position and quantity. The following are subject to mandatory removal:
- baby teeth that interfere with normal growth and formation of permanent teeth;
- strongly dystopic structures - located on the palate or at a large angle to the lateral side of the gums;
- impacted formations that put pressure on the adjacent roots of normal teeth and provoke periodic inflammatory processes of soft tissues.
If the additional tooth does not cause discomfort and does not disrupt the development of the dentition, removal may not be necessary. Moreover, such a superset can play the role of a strategic reserve in case of damage to nearby normal teeth.
How does the removal work?
The removal procedure can be simple or complex. In the first case, the doctor is dealing with a fully erupted tooth, the root of which is not intertwined with the surrounding structures. Simple removal steps:
- The oral cavity is prepared - treated with antiseptics, anesthesia is given.
- Grasp the crown with forceps (in some cases, an additional incision of the mucous tissue is required to facilitate access).
- The elevator destroys the retaining ligaments.
- The root is freed and the tooth is removed.
- Clean the hole from tooth fragments and bones.
- Apply stitches (if necessary) and a healing bandage.
Complex extraction is prescribed in the case of impacted, semi-impacted or dystopic teeth with complex root shapes. The procedure is carried out with a deep incision of soft tissues, in especially severe cases - with opening of the jaw bone to gain access to the roots. The latter option is relevant for deep bone occurrence, position in close proximity to the cranial sinuses and orbits, as well as for irregularly shaped roots and a high risk of damage to complete teeth. A complex removal operation is performed by a dental surgeon.
Price
Our Center operates a case payment system, which guarantees patients no overpayments for additional services associated with implantation.
The implant installation case includes:
- cost of Nobel Biocare implants;
- doctor's work;
- consumables and superstructures;
- anesthesia;
- CT diagnostics before and after surgery;
- fixation of bone regeneration stimulators (up to 0.25 cm³) to the neck of the implant for simultaneous bone tissue growth in conditions of slight atrophy;
- antibiotics and painkillers at home;
- visits according to schedule.
The case for installing crowns and bridges includes:
- fixation of abutments;
- taking impressions;
- manufacturing, installation of crowns or bridges.
Sinus lifting and guided bone regeneration, if necessary, are paid separately.
Orthodontic treatment
Depending on the situation, it is used after tooth extraction or instead of it. In children, it is used to stimulate the loss of baby teeth and eliminate false hyperdontia, as well as to facilitate and accelerate the eruption of a normal set. In addition, orthodontic treatment with the installation of braces, mouth guards, dental plates or other auxiliary structures can straighten crooked teeth and return them to their proper place.
Before prescribing treatment, the dentist carefully evaluates the condition of the complete and supernumerary structures and, depending on the overall picture and prognosis for the future, can use both formations or leave the strongest and most durable tooth (not necessarily complete).
Forward to the future!
Of course, there is no doubt that dental bioengineering will soon become an integral part of standard protocols for the treatment of dental lesions. It is possible that regenerative dentistry techniques will allow us to create a complete dentogingival complex. It is important to remember that methods developed in accordance with the requirements and objectives of dental bioengineering will be able to spur the development of new approaches to the regeneration of other tissues and organs and thus contribute to progress not only in dentistry, but also in the field of regenerative medicine in general. Well, forward to the future!