Alveolitis: classification
Diffuse lung damage exists in several forms:
- idiopathic fibrosing alveolitis. A complex term that combines pulmonary fibrosis and a group of chronic pneumonias. Quite a rare disease. According to the International Classification of Diseases (ICD-10), it has code J84. It affects the connective tissue of the lungs, subsequently developing pneumofibrosis and respiratory failure, and also increasing pressure in the pulmonary circulation. Inflammatory effusion accumulates in the alveoli, the lungs acquire a dense consistency and turn red;
- exogenous allergic alveolitis. It occurs as a reaction of the immune system to external stimuli (exogenous antigens). A phenomenon called “farmer's lung” is often observed, which is characterized by pulmonary edema, infiltration of organ tissue with lymphocytes and neutrophils. Typically, this syndrome is characteristic of persons who have inhaled hay mold, which contains actinomycete spores. With a long course of the disease, transformation of the lung tissue according to the “honeycomb” type is possible;
- toxic alveolitis. This pathological condition is caused by the entry of toxic substances into the respiratory organs, both aerogenously and through the bloodstream. The most important role in pathogenesis is played by individual intolerance to the traumatic substance.
Alveolitis of the lungs in children develops gradually, most often manifesting itself at an early age.
Alveolitis of the tooth has a code according to ICD-10 K10.3. There are:
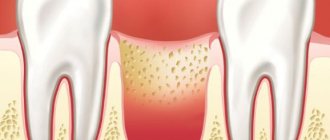
- acute form of the disease. In this condition, severe pain and swelling of the gums occurs; usually painful manifestations begin soon after tooth extraction;
- chronic form. It occurs a few days after tooth extraction; suppuration forms in the socket, which increases in size over time.
Alveolitis causes
Forms of pulmonary disease are characterized not only by various symptoms, but also by factors that contribute to the development of the disease:
- dust, mold, protein antigens, food products lead to the formation of allergic alveolitis. A special risk group consists of workers of chemical and pharmaceutical enterprises;
- viruses, smoking, and the entry of gastric contents into the bronchi contribute to the development of idiopathic fibrosing alveolitis;
- antibiotics, antitumor drugs, nitrofurans, oxygen during prolonged inhalation, hexamethonium, cordarone - an incomplete list of substances that can cause toxic alveolitis.
Alveolitis of the tooth socket usually occurs for several reasons:
- poor-quality treatment of the hole with antiseptics after tooth extraction;
- smoking;
- tooth alveolitis sometimes develops after complex extraction;
- improper oral hygiene;
- close proximity of teeth damaged by caries to the extraction site;
- immune disorders.
Alveolitis complications
Complications of the idiopathic fibrosing form usually occur in the case of an aggressive course of the disease (acute alveolitis) and include:
- oxygen deficiency in the body;
- pulmonary artery hypertension;
- transformation of the focus of the disease into malignant neoplasms;
- development of secondary infection and pneumonia;
- heart failure.
Complications of exogenous allergic alveolitis can be avoided by ceasing contact with the allergen. Otherwise, the following phenomena may occur:
- pulmonary artery hypertension;
- heart failure;
- respiratory failure.
A long course of toxic alveolitis is fraught with the development of pathological phenomena associated with the pulmonary system. These include:
- insufficient gas exchange;
- pathologies of the heart muscle;
- hyperventilation of the alveoli.
Dental alveolitis causes acute pain in the patient, so going to the hospital usually occurs soon after the onset of symptoms. In the absence of therapy, the following is observed:
- purulent inflammation of the oral cavity - phlegmon;
- osteomyelitis;
- blood poisoning.
Prevention and prognosis of alveolitis
To avoid the development of fibrotic lung disease, it is recommended:
- stop smoking;
- promptly treat bacterial and viral infections;
- Avoid harmful substances (silicates, asbestos, metal and wood shavings and dust).
The prognosis of the disease depends on the form of the process:
- the fulminant form is characterized by aggressiveness of the disease and a high percentage of deaths;
- the prognosis of the acute form is also unfavorable. Sometimes death can occur after 1-2 months;
- the chronic form is characterized by frequent relapses and irreversibility of the process. Average life expectancy is 5 years.
Exogenous allergic alveolitis can be prevented by following several rules:
- ventilate the premises well;
- observe hygiene standards when keeping animals;
- promptly replace filters in air conditioners;
- change profession when the first symptoms of the disease appear.
When the allergen is eliminated, the prognosis is favorable. Acute alveolitis, if treatment is started on time, does not cause long-term impairment of respiratory function. With a chronic disease, pneumosclerosis and respiratory failure develop, treatment is ineffective.
The main method of preventing the development of toxic pulmonary lesions is a favorable environmental situation and safe therapeutic therapy.
When the traumatic factor is eliminated, healing soon occurs. With constant exposure to the pathogen, life expectancy does not exceed 6 years.
To prevent inflammation of the socket, the following is recommended:
- refrain from physical activity for 24 hours after tooth extraction;
- Avoid hot food during the day after extraction;
- do not chew food with teeth located near the extraction site;
- do not touch the hole with dirty hands.
The prognosis of dental alveolitis is usually favorable, the patient becomes functional on the second day.
Description of the disease
Not all dental surgeon patients know that inflammation may develop after removal, so they often ask the question: “Alveolitis - what is it, and why does it occur?” Other names for the disease: “dry socket”, “alveolar local osteitis”. The pathogenesis of the condition is based on a violation of the formation of a physiological clot or its loss from the socket after tooth extraction, which most often occurs due to a violation of the postoperative regimen or low human immunoresistance.
Inflammation of the alveoli is possible only due to removal of the segment. Alveolitis cannot develop after tooth treatment, since the hole is formed only as a result of extraction of the unit.
Diagnostics
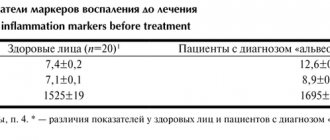
The development of complications after tooth extraction may be indicated by the following signs of alveolitis: pain that appears 3-5 days after tooth extraction, as well as a non-healing hole wound. A more accurate diagnosis can only be made on the basis of a carefully collected anamnesis, as well as laboratory and instrumental studies. In parallel, a differential diagnosis of alveolitis is carried out with allergic pneumomycosis, sarcoidosis, pulmonary eosinophilia, interstitial lung diseases, as well as collagenosis, which is detected on the basis of physical data.
Idiopathic form - ELISA
Diagnosis of ELISA is carried out on the basis of visual examination data, as well as results obtained after laboratory, radiological and functional examination methods.
Idiopathic fibrosing alveolitis is characterized by an increase in ESR in the blood, an increase in the concentration of CEC, as well as antinuclear bodies. X-rays can reveal changes and intensification of the pattern of the lung, and at a later stage - “honeycomb lung”, in which stringy compactions intertwine with zones of clearing. Based on the results of functional tests, pulmonary ventilation disorders of the restrictive type, arterial hypoxemia, and progression of the decrease in diffuse lung activity are determined.
To clarify the origin of morphological changes, a transthoracic or transbronchial biopsy of tissue from the affected lung is performed. Based on the examination of the fluid, the presence of lymphocytes, eosinophils, neutrophils, and macrophages is revealed, and the nature of the inflammation is clarified. Differential diagnosis is carried out with bronchopneumonia, pneumoconiosis, pulmonary tuberculosis and even bronchoalveolar cancer.
Exogenous form – EAA
Exogenous allergic alveolitis belongs to the category of diseases of an immunopathological nature that develop under the influence of organic dust containing specific antigens that cause diffuse lung damage.
The development of EAA is observed in patients who do not suffer from atopic reactions, but complain of worsening their condition after contact with the allergen, and who have a clearly defined clinical picture of the disease. Thus, the presence of increased ESR, C-reactive protein and leukocytosis is determined in the patient’s blood. X-ray examination reveals an increase in the pulmonary pattern, the presence of small focal shadows, and a decrease in the transparency of the tissue of the affected lung.
To make a diagnosis of alveolitis, radioimmunological, enzyme immunoassay, and immunofluorescence research methods are performed. In some cases, allergy tests, both skin and inhalation tests, are performed. Differential diagnosis of alveolitis is carried out with sarcoidosis, ELISA, pneumonia of an infectious nature, pulmonary fibrosis, which may be indicated by a cellular deformation of the lung pattern. The study of external respiration functions allows us to identify possible insufficiency of pulmonary ventilation of a restrictive type, accompanied by insufficient gas exchange and a violation of ventilation-perfusion relationships.
The most sensitive imaging method is CT of the alveolitis. It allows you to identify nodular opacities, areas of “ground glass”, and a “honeycomb structure” of lung tissue. An x-ray can show both a normal picture of the lung condition and a picture of severe pneumosclerosis.
Toxic form - TFA
Toxic fibrosing alveolitis is a diffuse lung lesion that develops under the influence of harmful toxic chemicals. An x-ray of the alveolitis does not show any changes in the organs of the thoracic region, however, in the later stages, diffuse enhancement of the pattern of the lung and its slight deformation may appear, and less commonly, diffuse fibrosis.
The study of external respiration functions allows us to identify insufficient ventilation of the lungs, hypoxemia, and a decrease in residual lung capacity. The formation of fibrous tissue, which actively replaces damaged epithelial tissue, indicates the progression of the disease, which can lead to the loss of the alveoli of their basic functions.
Toxic alveolitis is characterized by the absence of immunological pathologies, however, there are characteristic changes in the hemogram and biochemical tests, which can be caused by various pathological conditions developing against the background of the underlying disease. Differential diagnosis is carried out with ELISA, EAA, and sarcoidosis.
The main reasons for the appearance of alveolitis after tooth extraction
Tooth extraction is a surgical procedure that is accompanied by the formation of a wound. A blood clot forms in it, protecting it from the penetration of microorganisms. Inflammation of the tooth socket after extraction occurs due to disruption of the process of formation or displacement of a blood clot. The most common causes of pathology:
- Difficult extraction. The more traumatic the operation, the more the tissue’s ability to regenerate decreases and the likelihood of infection increases.
- Wisdom tooth removal. The structure of the root system of third molars is complex, so their extraction is always traumatic. In addition, the bone in the figure eight area has increased density and is less vascularized compared to other areas, which also creates conditions for the formation of a dry socket.
- Concomitant somatic diseases of the patient (diabetes mellitus, immunodeficiency states).
- History of pericoronitis (inflammation of the soft tissues around the tooth).
- The presence of foci of infection in the mouth before surgery. Penetrating into the wound with saliva, pathogenic flora causes alveolitis.
- Inadequate sanitation of the alveoli. After removal, careful curettage of the wound is necessary to remove fragments of bone tissue, roots, pieces of filling, and granulations. Foreign fragments disrupt healing and lead to alveolitis.
- Exceeding the dose of anesthetic. Leads to a narrowing of the lumen of the capillaries, the development of local ischemia, which disrupts the filling of the hole with blood.
- Mechanical damage to the clot. Failure to follow the doctor’s recommendations during the postoperative period (rinsing the mouth, carelessly brushing teeth, etc.).
- Impaired hemostasis. Due to poor blood clotting, a clot does not form.
Alveolitis can be provoked by smoking, taking hormonal contraception, and insufficient oral hygiene. Age plays a certain role in the development of alveolitis after tooth extraction: the older the patient, the greater the likelihood of developing pathology. This is due to a slowdown in metabolic processes and a decrease in the regenerative ability of tissue cells.
Symptoms of alveolitis of the socket
Alveolitis goes through several stages of development, each of which has its own clinical picture:
| Stage | Description |
| Serous inflammation | The first clinical symptoms appear the next day or after 3 - 4 days after surgery. Non-purulent inflammation is manifested by the appearance of episodic pain and swelling of the soft tissues around the alveoli. |
| Purulent alveolitis | If measures were not taken at the previous stage, a purulent process develops within a few days. The pain becomes constant, radiating to the auricle, jaw, and neighboring teeth. The infection spreads to nearby lymph nodes, causing them to enlarge. A gray-green coating appears inside the hole. The temperature rises. |
| Purulent-necrotic stage | The pain intensifies and becomes throbbing. A putrid odor appears from the mouth. Progression leads to disruption of microcirculation, ischemia, and the development of necrosis. The patient’s health deteriorates significantly, and signs of intoxication appear. |
| Hypertrophic tissue change | Lack of medical intervention within 14 days leads to chronicity of the process. Soreness and swelling become less pronounced. Soft tissues grow and fill the hole. When pressure is applied to the granulation, pus is released. The mucous membrane is swollen, bluish in color. |
If left untreated, alveolitis has an unfavorable outcome. The main complications after alveolitis:
- phlegmon (extensive purulent inflammation);
- acute periostitis (inflammatory process of the periosteum);
- osteomyelitis (purulent-necrotic inflammation of the jaw bone);
- sepsis (purulent-septic blood disease).
Medicines
If alveolitis has developed, medications are prescribed by a doctor. The selection of medications depends on the severity of the disease, as well as the spread of the inflammatory process. After removing the remains of the tooth and other particles remaining in the hole, apply a bandage with antiseptic agents. The patient is also advised to regularly rinse his mouth, change the bandage, or lubricate the gums with antiseptic or wound-healing drugs. They can be available in the form of a gel, cream or ointment, as well as rinses or aerosols.
In most cases, antibiotics are needed for alveolitis. The only exception may be a mild form of the disease. Often, the doctor prescribes drugs for local treatment containing antibacterial components. Metrogyl denta for alveolitis has not only an anti-inflammatory, but also an antiseptic effect. Thanks to the destruction of harmful bacteria, the healing process of the hole is accelerated.
For severe pain, which often accompanies the inflammatory process of the tooth socket, the patient is prescribed painkillers. This could be analgin or a potent drug (Nimesil, Nurofen, and so on). Some dental medications have an analgesic effect (Stomatidin).
Antiseptic drugs for alveolitis
The main goal of treating alveolitis is to relieve the inflammatory process and further prevent the proliferation of bacteria, viruses and fungi in the tooth socket. Treatment for this disease includes taking antiseptics. The doctor may prescribe one of these medications:
- Hexicon;
- Chlorhexidine;
- Maxicold Lore;
- Stopangin.
Chlorhexidine for alveolitis, like other medications in the form of a spray, should be applied 2-3 times a day after meals. Antiseptic solutions are used for rinsing the mouth, as well as lotions (a cotton swab is soaked in the solution and applied to the inflamed hole for half an hour). Hydrogen peroxide is also used for rinsing (1 tablespoon should be diluted in a glass of warm water).
Antiseptics in the form of a gel, for example, Hexicon, are applied in a thin layer to the inflamed gum around the hole. Many antiseptic medications have an analgesic effect, and Solcoseryl prescribed by the doctor for alveolitis will speed up the wound healing process.
Alveolitis and antibiotics
For alveolitis, the doctor may prescribe an ointment with antibacterial agents. In case of severe inflammation, antibiotics, as well as in cases where the risk of complications increases, can be prescribed in the form of tablets for oral administration. It could be:
- Ciprofloxacin;
- Clindacil;
- Metrogil.
Taking antibiotics allows you to quickly eliminate severe pain and other unpleasant symptoms. And within a few days the inflammatory process will be completely stopped.
Painkillers
Alveolitis is accompanied by severe pain, so the patient is prescribed painkillers. The doctor may prescribe:
- Analgin;
- Amidopyrine;
- Nurofen;
- Panadol.
Some painkillers have contraindications or a number of side effects, so a doctor should select the medications. He will take into account the severity of the disease, as well as the individual characteristics of the patient. The use of local anesthetics is considered effective. They are usually applied to cotton wool or gauze and applied to the hole.
But since the treatment of alveolitis of the socket is carried out with antiseptic and anti-inflammatory drugs, after a few days the pain becomes less severe, and then disappears completely.
Alveolitis after wisdom tooth removal
Indications for the removal of eighth segments in a row can be different: deep caries, improper eruption, orthodontic correction of jaw bite, dystopia, etc. Extraction of third molars is always associated with trauma to nearby tissues, which increases the development of inflammation. The pathological process is observed in 45% of cases due to the removal of lower wisdom teeth.
Symptoms of alveolitis after wisdom tooth removal are similar to the general symptoms of the disease. However, with such localization of inflammation, a sore throat and impaired functionality of the temporomandibular joint on the affected side may occur (difficulty and painful opening of the mouth).
Impacted tooth - symptoms and treatment
If the patient has no complaints, impacted teeth are usually identified as an incidental finding during an appointment with dentists of various specialties or orthodontists.[11]
The main reason for contacting a dental surgeon is acute pericoronitis, a condition in which patients notice sudden pain in the area of an erupting tooth while chewing. Usually the inflammatory process is localized in the gum area and the formed “hood” over the coronal part of the wisdom tooth.
During the examination, you can see a slight swelling of the patient over the “figure eight” (wisdom tooth) that has partially or completely appeared in the oral cavity, with a small amount of clear or slightly cloudy serous discharge, as well as without it. In this case, there is no swelling of the face or restriction in mouth opening. The regional submandibular lymph nodes may be enlarged and painful. Body temperature is within normal limits, and the patient's general condition is satisfactory. This form of the disease is called catarrhal and, as a rule, goes away quite quickly and favorably with timely treatment.[2][6][17]
If the process worsens and the form becomes purulent, patients note a deterioration in their health, increasing weakness, and an increase in body temperature to 38.0°C. The pain becomes constant and radiates to the temple, ear and back of the head from the side of the teething. Due to increasing swelling of the soft tissues, restriction and pain occur when opening the mouth - inflammatory contracture of the masticatory muscles. Patients note enlargement and pain in the area of the submandibular lymph nodes. In the oral cavity, swelling and redness of the soft tissues are observed not only in the area of the “hood” above the crown of the impacted tooth, but also in the area of the palatine arches and the mucous membrane behind the “eight”. Touch and palpation in this area are sharply painful, and suppuration is observed from under the hood. Adequate treatment of purulent pericoronitis also contributes to a favorable outcome.[4][6][17]
If acute inflammation occurs repeatedly in the area of impacted teeth with periods of improvement, we can talk about chronic pericoronitis. Patients also report pain in the area of the erupting tooth when closing the jaws and chewing. The mucous membrane of the “hood” already has scar changes, bedsores with aphthae or ulcers, which indicate a long course of the disease. Body temperature is usually normal and general condition is satisfactory. Under the “hood”, as a rule, there is a small amount of discharge with an unpleasant odor and taste. Pain and symptoms of periodontitis in the teeth adjacent to the impacted ones are possible. Chronic pericoronitis is characterized by frequent exacerbations.[2][4][6]
When teeth are impacted in the anterior region or in an aesthetically significant area, patients may complain about a lack of harmony in the dentition and dissatisfaction with their own smile. As a rule, in this case, tooth retention is accompanied by a combined dentofacial anomaly.[1]
Methods for diagnosing alveolitis
How long the alveolitis will take to heal depends on timely diagnosis and treatment. Therefore, at the first signs of illness, you should consult a dentist. Identification of pathology occurs after listening to complaints, collecting anamnesis (where there is recent tooth extraction) and examining the socket cavity.
Sometimes the doctor prescribes an x-ray examination, which helps to detect tooth fragments and other foreign fragments in the alveolus. In rare cases, when alveolitis of the tooth socket , computed tomography is prescribed for the purpose of differential diagnosis of other diseases (trauma, tumor, etc.).
How to treat alveolitis after tooth extraction
The main task of correction is aimed at eliminating the cause that caused the pathology and stopping the inflammatory process. The doctor decides how to treat alveolitis after tooth extraction. Treatment tactics depend on the stage of the pathological process. It may include revision (if necessary, curettage) of the hole, drug treatment, physical therapy (laser, magnet, fluctuarization, ultraviolet radiation). All manipulations are performed under local anesthesia.
Treatment program:
- Local anesthesia.
- Antiseptic treatment of the wound (removal of saliva, food debris, pus).
- Freeing the cavity from a disintegrated blood clot, foreign inclusions (tooth fragments, root remains, etc.), granular tissue.
- Repeated treatment with an antiseptic, application of a turunda soaked in an anesthetic drug.
- Applying a medicated antiseptic bandage.
When treating alveolitis, the doctor can use proteolytic enzymes (trypsin, chymotrypsin), which break down necrotic tissue, thereby helping to cleanse the socket. To reduce pain, a blockade is made with local anesthetics, which are injected into the soft tissue near the inflamed alveoli. To suppress the infectious process, a course of antibiotic therapy is prescribed.