Trigeminal neuropathy is a lesion of the trigeminal system, which is characterized by changes in the interstitial tissue, myelin sheath, axial cylinders and is manifested by pain, paresthesia and sensitivity disorders in the areas of innervation of its main branches. If the mandibular nerve is involved in the pathological process, chewing function is impaired.
Among the etiological factors of trigeminal neuropathy are the following:
- infectious (malaria, viral hepatitis, syphilis, tonsillitis, sinusitis);
- iatrogenic (as a consequence of destructive therapy);
- traumatic;
- ischemic;
- intoxicating.
Most often, neuropathy of individual branches of the trigeminal nerve is determined.
Neuropathy of the inferior alveolar nerve occurs during infectious diseases, diffuse osteomyelitis, dental procedures (introduction of an excess mass of filling material behind the apex of the tooth in the treatment of premolars and molars of the lower jaw, traumatic extraction of teeth, especially the third lower molars, performance of mandibular anesthesia), toxic periodontitis.
Clinic.
The leading symptoms are pain and numbness in the area of the lower jaw, chin, gums and lower lip. An objective examination reveals loss or reduction of all types of sensitivity in the gum area of the lower jaw, lower lip and chin on the affected side. In the acute stage, painful contraction of the jaws (trismus) in combination with paresis of the masticatory muscles can be observed.
In dental practice, sometimes there is acute toxic-traumatic neuropathy of the lower alveolar nerve, the mental one, which occurs when filling material gets into the mandibular canal during the treatment of pulpitis of the first and second premolar on the lower jaw. During canal filling, the patient acutely experiences very intense pain in the lower jaw with numbness of the lower lip and chin. If such a situation arises, emergency measures are taken - decompression of the canal: dexamethasone 8 mg + 5 ml of 2.0% aminophylline solution + 20 ml of 40% glucose solution intravenously. At the same time, diphenhydramine 1 ml intramuscularly and furosemide 40 mg intramuscularly are prescribed. Subsequently, agents are used that improve microhemocirculation (nicotinic acid, pentoxifylline), as well as neuroprotectors (nootropil, cerebrolysin, actovegin), desensitizing drugs (diphenhydramine, suprastin, diazolin).
Neuropathy of the buccal nerve.
The causes of the disease can be periostitis, inflammatory diseases of the teeth and gums, traumatic removal of teeth in the lower jaw.
Clinic.
The pain occurs subacutely, is constant, and its intensity gradually increases. First it occurs on the front surface of the gum, transitional fold, and then spreads to the entire front surface of the teeth of the lower jaw and covers the entire area of innervation of the buccal nerve. Numbness is uncharacteristic; an objective examination reveals a decrease in all types of sensitivity in the area of innervation of the mucous membrane of the cheek and vestibular surface of the gums, as well as the skin of the corner of the mouth.
Neuropathy of the superior alveolar nerve.
The causes of the disease may be chronic pulpitis and periodontitis, nerve damage in case of complex tooth extraction, sinusitis, and surgical intervention for sinusitis.
It manifests itself as pain and a feeling of numbness in the teeth of the upper jaw. Objectively, there is a decrease or absence of sensitivity in the gum area of the upper jaw, as well as the adjacent area of the buccal mucosa. The electrical excitability of the pulp in the corresponding teeth of the upper jaw is reduced or absent.
If the cause of the disease is stenosis of the infraorbital canal, then patients will complain of pain and numbness of the skin in the area of innervation of the infraorbital nerve (wing of the nose, area above the canine fossa, upper lip).
Factors influencing neurological response to nerve injury
— Preoperative screening for neuropathic pain is necessary. Preexisting neuropathic dental pain (PDAP type 1), which exists before surgery, can be caused by many different systemic conditions, medications, and other lesions. It is critical that surgeons recognize presurgical neuropathic conditions because neuropathic pain does not respond to surgery and can often lead to worsening pain. In addition, poorly controlled preoperative pain and nerve damage can cause chronic postoperative pain.
— The main indicators for predicting chronic post-surgical pain are psychological factors, including the level of anxiety, neuroticism (a fundamental personality trait in psychology, characterized by anxiety, fear, rapid mood swings, frustration and a feeling of loneliness. It is believed that neurotic people cope worse with stress and are prone to exaggerate the negative side of a particular situation.), catastrophization and introversion. Thus, the doctor has the opportunity not to perform the surgery of choice (implantation) in such patients, but to decide in favor of an alternative treatment plan.
- The concentration of the anesthetic used is up to 2% lidocaine - the accepted standard, because higher concentrations have a greater neurotoxic effect, which may cause permanent neuropathy. Avoid using multiple (repeated) anesthetic blocks in the same area for the same reason.
— Preoperative medical examination should exclude the following diseases : Raynaud's disease, Erythromelalgia (Mitchell's disease), Irritable bowel syndrome (IBS), Migraines, Fibromyalgia.
—Location of surgery is another factor associated with neurological response. Trauma in the distal jaw is more significant (eg, angle and ramus) than in the mental foramen, because the closer the proximal nerve injury is, the greater the risk of damaging trigeminal ganglion cells and initiating retrograde effects of differentiation into the central nervous system. .
Thus, a thorough interview and examination of the patient, detailed pre-implantation planning based on CBCT data, appropriate visualization of the implantation plan and the use of surgical guides, selection of optimal implant sizes with extended safety zones, use of drill limiters and, of course, an experienced team of doctors who will carry out the implantation followed by early postoperative care, all of which will contribute to safer practice and optimized patient outcomes.
Traumatic neuropathy. Etiology.
Traumatic neuropathy most often occurs in the case of surgical interventions on teeth (traumatic extraction of teeth, removal of filling material beyond the apex of the tooth root, anesthesia with injury to the nerve trunks, removal of bone or tumor of the jaws), as well as in cases of surgical interventions on the paranasal sinuses and infraorbital canal.
Damage to the first branch of the trigeminal nerve, as a rule, is practically not observed. Most often, the third branch of the trigeminal nerve is affected, which is apparently due to the anatomical location of the inferior alveolar nerve, which makes it easily accessible during a variety of traumatic dental procedures. This is especially true for dental interventions on third molars. The cause of traumatic neuropathy of the inferior alveolar nerve can also be filling the mental canal during the treatment of pulpitis of the 4th and 5th teeth of the lower jaw.
Combined damage to the I and II branches of the trigeminal nerve can occur after inflammatory diseases of the brain with the development of adhesions or in the case of sinusitis, when the maxillary and frontal sinuses are simultaneously involved in the inflammatory process.
Clinic.
Patients complain of constant aching, sometimes pulsating pain in the area of innervation of the injured nerve, a feeling of numbness and “crawling goosebumps”. In case of injury to the mandibular nerve, tooth alignment occurs, which is associated with damage to the motor part of the nerve; patients cannot eat or talk. Trigger zones on the face and in the oral cavity are not identified.
During an objective examination, hypoesthesia or anesthesia (hyperpathy is also possible) of the skin and mucous membrane in the area of nerve innervation is detected. On palpation, pain is noted at the exit points of the II and III branches of the trigeminal nerve, as well as in the case of vertical percussion of the teeth and deep palpation of the lower jaw.
Diagnostics.
The main diagnostic criterion is the occurrence of pain after interventions on the dental system. The disease is characterized by clinical polymorphism and significant duration. During weather changes, stressful situations and in the presence of somatic diseases, exacerbation of the pain syndrome may occur.
In the event of scar changes in the nerves or retraction of the nerve into the scar of soft tissues (after gunshot wounds, in the case of defects of soft and bone tissues after resection of the jaws), constant aching pain of unexpressed intensity with persistent sensory disturbances is observed.
Causes
The NAN is damaged not only during the installation of implants, but this is the main reason. In addition to unsuccessful implantation of an artificial root, the nerve suffers in the following cases:
- extraction of incorrectly located wisdom teeth in the lower row;
- penetration of the composite material into the canal with the nerve;
- improperly performed conduction anesthesia.
Infectious diseases and inflammatory processes with suppuration also often threaten the integrity and full functionality of the inferior alveolar nerve.
Iatrogenic trigeminal neuropathy.
This nosological entity arose due to the fact that treatment of trigeminal neuralgia in most cases began with neurodestructive operations (alcohol-lidocaine blockades, neuroexeresis, destruction of the trigeminal ganglion). As a result, a significant number of patients experienced iatrogenic traumatic or toxic-traumatic neuropathies of the trigeminal nerve. The maxillary and mandibular nerves were most often affected.
In many textbooks on neurology, in case of trigeminal neuralgia, it is proposed to carry out alcohol-novocaine and alcohol-lidocaine blockades of its peripheral branches or node - the so-called alcoholization . The analgesic effect in this case is achieved on average after the second or third procedure, but it is explained by the fact that numbness occurs due to the development of destructive changes in the nerve trunk. Over time, toxic-traumatic neuropathy develops, practically resistant to treatment, so the patient must continue to undergo blockades, the effectiveness of which decreases in proportion to their number.
Thus, neurodestructive operations that are performed in the treatment of neuralgia lead to the development of toxic-traumatic neuropathy. This determines the nature of the pain syndrome.
Clinic.
The clinical picture is usually represented by the presence of constant aching, burning or dull neuropathic pain in the area of innervation of the affected nerve, against the background of which neuralgic paroxysms occur with irradiation of pain, respectively, to the segmental areas of the face (Zelder segments). Patients experience various types of paresthesia (numbness, crawling, burning) and sensitivity disorders (hypesthesia with symptoms of hyperpathia or hyperesthesia), which sometimes spread beyond the innervation of one of the branches of the trigeminal nerve.
In many cases, vegetative fibers are drawn into the process, which leads to trophic changes in the oral mucosa (gingivitis), the dental system (progressive periodontitis) and facial skin (pigmentation or depigmentation, dryness, peeling, soft tissue atrophy). In such cases, the pain becomes unbearably burning, tearing, boring, and is accompanied by vegetative reactions (redness and swelling of the facial skin, local increase in body temperature, lacrimation, salivation).
During neurodestructive manipulations on the mandibular nerve, painful contraction of the teeth may occur (patients are forced to eat through a straw and cannot speak or open their mouth). With each subsequent alcoholization, the nature of the pain syndrome changes: neuralgic paroxysms become longer, more frequent, a neuralgic status can form, and slightly pronounced trigger areas appear on the skin of the face. Pain is provoked by weather conditions (cold or heat), exacerbation of somatic pathology, food consumption, and physical activity. The exit points of the trigeminal ditch are painful during palpation in approximately 2/3 of patients.
The data presented convincingly indicate that neurodestructive manipulations are not the method of choice for the treatment of trigeminal neuralgia, since in most cases a short-term effect is achieved. However, such therapy leads to the development of toxic neuropathy, disease progression and the development of resistance to conservative treatment methods. Only when all the methods used to treat neuralgia are not effective, and the intensity of the pain syndrome remains severe, can neurodestructive operations recently developed by neurosurgeons be used.
Clinical algorithm for determining post-traumatic neuropathy
Trigeminal Neuropathy Assessment Questionnaire
Important! Severe pain experienced during treatment may indicate a possible nerve injury.
- History of the initial onset of pain.
- Development of pain.
- Duration of pain.
- History of regular pain SOCRATES (Site, Onset, Character, Radiation, Associated signs, Timing, Exacerbating and relieving factors, Severity) - Localization, Occurrence (frequency of attacks), Character, Irradiation, Associated symptoms, Duration, Exacerbation and relief factors (what intensifies and relieves pain), severity of pain.
- Psychological screening.
- Functional screening (impact on daily life).
Mechanosensory tests (mapping the affected area)
A protocol for examining the dermatome to assess the extra-oral mechanosensory function of the alveolar branch of the trigeminal nerve.
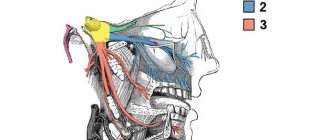
Dermatomes are segments of skin into which the entire surface of the human body is divided in connection with its innervation by various roots of the spinal cord, in this case the trigeminal nerve.
Figure 7. Dermatomes of the branches of the trigeminal nerve
1. Logging the affected area.
Using surgical forceps, move from the normal to the neuropathic (changed) area, warning the patient that there may be increased sensitivity and/or decreased sensitivity. Mark an area on the patient's face with marker marks and take a photo. Assess the % or area of the extra-oral dermatome that is affected by neuropathy.
2. Recording the assessment of subjective sensation.
Press the surgical forceps or probe firmly (but not painfully) against the patient's arm several times at intervals (5 times per minute), explaining that this is a "normal" subjective rating of function on a scale of 10 out of 10. Press with the same pressure on the unaffected side of the face or tongue and repeat the stimulation, explaining that it should be 10 out of 10. Then remove the forceps or probe and explain that the missing stimulation is 0 out of 10. Only then repeat the same actions in the area of neuropathy that you have already confirmed and marked with markers labels, and ask the patient to report the stimulus level out of a possible 10 (if >10 = hyperesthesia and <10 = hypoesthesia). This test should be repeated in different areas of the neuropathy (lip border, lip skin, chin, tongue, etc.)
3. Recording the light touch assessment
To assess light touch thresholds, it is recommended to use a frayed cotton swab, repeating touches at intervals of 5 times per minute. First on the unaffected side and then repeating on the affected side, ask the patient to report the differences. If the patient is experiencing numbness, then the stimulation will have a reduced threshold for detecting light touch, however, if the patient suffers from hyperesthesia and possible allodynia (pain to touch), then this test can be very uncomfortable and irritating.
Dermatomal Involvement Map Interpretation and Neuropathy Assessment —Does the area of neuropathy correspond to the dermatomal area in which surgery was performed? — Dynamics of the area of the involved extraoral and intraoral area when mapping neuropathic areas (criterion reliability is low)
Important! Localized sensory neuropathy is not always present in patients, but there is almost always an area of abnormal sensation, and the patient's maximum pain is associated with the area of sensory deficit, that is, suffering from a combination of pain, numbness and altered sensation. This is an important diagnostic distinction for sensory neuropathy.
Subjective function
- Is neuropathy hyperesthesia or hypoesthesia?
- Thermal allodynia test is the occurrence of pain when exposed to heat or cold. Thermal allodynia, especially cold allodynia, is a feature in patients with trigeminal nerve damage.
- Thermal hyperalgesia test. Increased pain that occurs after a weak stimulus.
- Test "Direction of movement". The patient closes his eyes, the doctor uses a soft brush to determine the patient's ability to detect both the sensation and the direction of movement of the brush.
- Test for sensitivity to temperature stimuli. A cotton swab with cold test spray and a dental mirror handle heated to 43 - 45 ° C are used to determine the patient's ability to feel cold and heat. Alternatively, test tubes can be filled with hot (43 -45 °C) water and cold water.
There are WHO recommendations regarding which parameters of peripheral sensory consequences should be taken into account to predict the results of microsurgical restoration of a damaged sensory nerve. Zuniga JR and Yates DM adapted the recommendations to trigeminal nerve lesions. More details here: Zuniga JR and Yates DM Factors Determining Outcome After Trigeminal Nerve Surgery for Neuropathic Pain. J Oral Maxillofac Surg 2021 Jul;74(7):1323-9.
Today, a guideline for mandatory X-ray monitoring after endodontic treatment and dental implantation surgery has already been adopted in order to indicate the relationship between the root and the root filling, as well as the proximity of the implant bed and/or the implant itself to the canal of the inferior alveolar nerve. Intraoral dental radiography is considered to be sufficient to detect iatrogenicity, although post-traumatic neuropathy is primarily a clinical diagnosis.
Renton T, Yilmaz Z. Managing iatrogenic trigeminal nerve injury: a case series and review of the literature. Int J Oral Maxillofac Surg 2012 May;41(5):629-637.